Folinic Acid in Non-Verbal Children: Mechanisms and Clinical Considerations
1. Mechanisms of Folinic Acid in the Brain and Speech Development
For folate to support speech and brain development, it must reach the brain in its active form. Folinic acid (5-formyltetrahydrofolate) plays a unique role in bypassing certain metabolic and transport limitations.

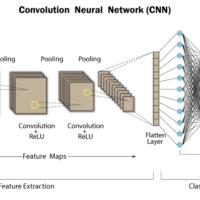
Mechanism of folate transport across the blood–brain barrier. Folinic acid (5-formyl-THF) is efficiently metabolized to 5-MTHF and transported into the CSF via the reduced folate carrier (RFC), even when folate receptor alpha (FRα) function is impaired. This allows folinic acid to bypass blockages in folate transport. In contrast, excess synthetic folic acid can bind with high affinity to FRα at the choroid plexus and is not readily converted to active folate in humans. Unmetabolized folic acid may thus competitively inhibit 5-MTHF transport into the brain, making folinic acid a more effective way to supply folate to the CNS.
Folate Metabolism and Neurotransmitters: Folate is crucial in one-carbon metabolism, which affects DNA methylation, myelination, and neurotransmitter synthesis. In the brain, the active folate 5-methyltetrahydrofolate (5-MTHF) is required as a cofactor for converting homocysteine to methionine (producing S-adenosylmethionine, the universal methyl donor). Adequate methylation is necessary for the production of monoamine neurotransmitters and for myelination processes. Folate is also tied to tetrahydrobiopterin (BH4), an essential cofactor for synthesizing serotonin, dopamine, and norepinephrine. When cerebral folate is low, BH4 levels can drop, impairing these neurotransmitter pathways. This biochemical impact suggests why folate deficiency might specifically affect cognitive and language development.
Transport into the Brain: Under normal conditions, 5-MTHF from the bloodstream enters the brain by binding to folate receptor alpha (FRα) on the choroid plexus. In some children, this pathway is impeded – either by autoantibodies against FRα or by genetic issues – leading to low folate in cerebrospinal fluid (CSF) despite normal blood folate. Folinic acid (which is 5-formyl-THF) can help in two ways: (1) it can be converted (via the enzyme MTHFD) to 5-MTHF in the gut and liver, thereby providing the active folate form; and (2) at high doses it can utilize the reduced folate carrier (RFC)transport system to enter the brain. RFC is a lower-affinity transporter that can ferry reduced folates (like folinic acid) across the blood–brain barrier if the concentration in blood is high. Essentially, high-dose folinic acid “floods” the system, so enough active folate reaches the brain even if FRα is partially blocked. This mechanism underpins folinic acid therapy for certain children with autism or developmental delays who have folate transport issues.
Effects on Speech Development: Speech and language are complex functions that require optimal neural development and neurotransmitter function. If folate-dependent processes (methylation, monoamine neurotransmission, etc.) are impaired in the developing brain, a child may experience delays in speech acquisition. By restoring normal folate levels in the CNS, folinic acid may improve neuronal communication and synaptic plasticity underlying language. Additionally, some non-verbal children may have undiagnosed cerebral folate deficiency that specifically dampens linguistic progress – treating them with folinic acid can unleash previously stymied development. For example, clinical cases report that toddlers with severe speech apraxia and folate receptor autoantibodies began gaining words when treated with high-dose folinic acid. The rationale is that folinic acid rescues the brain from a functional folate starvation, thereby normalizing the neurochemical environment needed for speech.
Clinical Evidence in Autism: Several studies support folinic acid’s benefits for language in autism. A pivotal randomized controlled trial (Frye et al., 2016) showed that 12 weeks of high-dose folinic acid (2 mg/kg/day, up to 50 mg) significantly improved verbal communication in children with autism and language impairment compared to placebo. Notably, the greatest improvements were seen in those children who had folate pathway abnormalities, such as the presence of folate receptor autoantibodies (FRAA). In an earlier open-label study, children with autism who tested positive for FRAA demonstrated gains in receptive and expressive language, attention, and stereotypical behaviors when given folinic acid supplements. These improvements are thought to result from correcting an underlying cerebral folate deficiency in a subset of autistic children. Indeed, FRAAs are found in a high proportion of children with autism (~70–75% in some cohorts), and those with these antibodies are the ones who tend to respond best to folinic acid therapy. Beyond autism, folinic acid is standard therapy in classic cerebral folate deficiency syndrome (a condition causing severe developmental regression) – when administered early, it can reverse neurological symptoms and allow children to regain skills, including speech. Thus, folinic acid’s mechanism of action (overcoming folate transport blocks and replenishing brain folate) directly translates to functional gains in communication for those children whose speech delay stems from or is exacerbated by folate-related metabolic problems.
2. Cerebral Folate Transport Deficiency (CFTD) vs Autism Spectrum Disorder
What is CFTD? Cerebral Folate Transport Deficiency, often used synonymously with cerebral folate deficiency (CFD) syndrome, refers to any condition where 5-MTHF levels in the brain (CSF) are abnormally low despite normal folate levels in blood. The most well-known causes are:
- Folate receptor α (FRα) autoantibodies: An autoimmune reaction that blocks folate transport into the brain. This is found in many cases of autism-related CFD.
- FOLR1 gene mutations: Rare biallelic mutations in the gene encoding FRα, leading to a dysfunctional transporter (fewer than 20 cases documented). This is the classic FOLR1-related CFTD.
- Mitochondrial or other metabolic disorders: For example, Kearns–Sayre syndrome can secondarily cause low CSF folate.
In CFTD, the infant is born healthy and has normal peripheral folate, but between 4–6 months and 2 years of age, as brain folate stores deplete, symptoms emerge. The clinical picture of infantile CFD was first described by Ramaekers et al.: affected children typically show irritability, developmental regression, movement disorders (tremor, ataxia, spasticity), and often epileptic seizures in early childhood. Notably, language loss or lack of speech is a prominent feature – many CFD children become non-verbal or never develop normal speech. They may also exhibit autistic-like behaviors (poor eye contact, social withdrawal, repetitive movements), which means CFD can phenotypically mimic autism. However, there are important distinctions between idiopathic autism and CFTD:
- Underlying Cause: Autism spectrum disorder (ASD) is behaviorally defined and biologically heterogeneous – no single metabolic deficit accounts for it. CFTD, in contrast, has a defined biochemical basis: insufficient folate in the CNS, often due to a transport defect. In practice, this means CFTD is potentially reversible (with folinic acid) whereas autism is not “reversible” in the same way, though some autism symptoms might improve if the child indeed has an underlying folate issue.
- Neurological Involvement: CFTD almost always involves neurological abnormalities beyond autism traits. For instance, hypotonia (low muscle tone), coordination problems, and seizures are common in young children with CFD syndromes. Autism by itself typically does not cause motor coordination loss or early-onset seizures (only about 20% of children with idiopathic ASD develop seizures, usually later in childhood or adolescence). Thus, a toddler with autistic features and clear neurological motor signs or frequent seizures should raise suspicion of an underlying CFTD or other metabolic disorder rather than autism alone.
- Onset and Regression: In idiopathic ASD, parents often notice developmental differences within the first 1–2 years of life (e.g. lack of babbling, reduced response to name) or a plateau/regression around 18–24 months. In CFTD, there is often a more dramatic regression after a period of normal development. For example, a baby might develop normally for 5–6 months, then start losing skills (e.g. stops babbling or making eye contact) as the brain folate drops. The regression in CFTD can be severe, including loss of motor skills, whereas in autism the regression (if it occurs) usually affects social and communication skills predominantly.
- Behavioral Profile: Children with CFTD can display autistic behaviors, but they often also have extreme irritability and sleep disturbances that stem from neurological distress. They may cry inconsolably (an expression of neurological pain or headache due to low folate) – a symptom less typical in standard autism. Also, autistic features in CFTD are often accompanied by cognitive stagnation or decline, whereas many autistic children continue to make cognitive gains even if their social communication is impaired.
- Biomarkers: By definition, CFTD features a low CSF folate level (< 5 nmol/L of 5-MTHF, often markedly low). Many children with autism have normal CSF folate (unless they coincidentally have CFTD). Additionally, around 75% of idiopathic autism children test positive for serum FRα autoantibodies in some studies, but this high rate likely reflects a subset who have “autoimmune folate deficiency” contributing to their autism. In contrast, such antibodies are found in only ~10% of typically developing kids. So a positive FRα antibody test strongly suggests CFTD or at least folate-related pathology in an autistic child. (By comparison, there is no “autism antibody” test – autism diagnosis doesn’t rely on lab tests.)
- Treatment Response: Perhaps the most striking difference: CFTD is treatable with high-dose folinic acid. Children with CFTD often show improvement (sometimes dramatic) in symptoms once on folinic acid for a few months. For example, they may start gaining or regaining speech, improve muscle tone, and have reduced seizures. In idiopathic autism, folinic acid is not a guaranteed treatment – it helps a subset (particularly those with FRAA) but many autistic children without folate issues will not respond to folinic acid. Autism interventions are largely educational and behavioral, whereas CFTD is a medical condition that can be directly addressed pharmacologically.
Below is a comparative table summarizing key differences and overlaps between Cerebral Folate Transport Deficiency (CFD/CFTD) and non-syndromic Autism Spectrum Disorder:
| Feature | CFTD (Cerebral Folate Deficiency) | Idiopathic Autism |
|---|---|---|
| Etiology | Typically caused by impaired folate transport to brain – e.g. folate receptor α autoantibodies or rare FOLR1 gene mutations. | Heterogeneous; no single cause (genetic and environmental factors; not linked to folate transport). |
| Onset and course | Normal early development followed by regression between ~5–24 months as brain folate falls. Progressive neurological deterioration if untreated. | Symptoms usually evident by ~2 years (may be earlier subtle signs); some cases show regression at 1–2 years, others have early delays. Typically a lifelong condition (developmental course can improve with therapy but core autism tends to persist). |
| Speech and communication | Often severely affected – may be non-verbal or lose words after early development. Folate deficiency can specifically impair language development; many CFTD cases have marked speech apraxia or delay. | Ranges from non-verbal to only mildly impaired; deficits in communication are a core feature of ASD, but outright loss of previously acquired words (regression) happens in a subset. |
| Social interaction | May appear autistic (poor eye contact, social withdrawal), especially during regression, but often accompanied by neurological signs like irritability or agitation beyond typical autism behavior. | Core social deficits: lack of typical eye contact, difficulty understanding social cues. No underlying metabolic upset assumed. |
| Neurological findings | Frequently present: hypotonia (low muscle tone), abnormal motor coordination or gait (ataxia), and seizures in many cases. Head growth may slow (acquired microcephaly). Irritability and sleep disturbances common. | Usually neurologically normal on exam (no consistent muscle tone or reflex abnormalities). ~20–30% have seizures, mostly starting in adolescence rather than infancy. No specific MRI abnormalities in most cases (aside from those due to co-existing conditions). |
| GI and feeding issues | Feeding difficulties in infancy are common in classic CFD syndrome; can include feeding aversion or failure to thrive. (In FRα autoimmunity, many children also have milk intolerance, since dairy can trigger antibodies.) | Many ASD children have GI issues (e.g. reflux, constipation, or picky eating) but not due to folate transport – often functional or due to sensory food aversions. Gluten/casein sensitivity can occur but is variable. |
| Diagnostic tests | Low 5-MTHF in CSF (by lumbar puncture) is the hallmark. Serum folate may be normal. Folate receptor α blocking antibodies often elevated in blood. If genetic, biallelic FOLR1 mutation found on molecular testing. | No definitive lab test; diagnosis is clinical. Genetic testing (chromosomal microarray, etc.) often done to find associated mutations (e.g. some syndromic forms). Metabolic workup is typically normal (folate levels in blood/CSF are normal in most autistic children, except those with coexisting CFD). |
| Treatment | High-dose folinic acid (leucovorin) to bypass transport problem, often long-term. Response can be dramatic if started early: improvements in motor skills, seizures, and communication are documented. Adjunct: remove dairy (to reduce antibody stimulation) and sometimes immunotherapy (e.g. corticosteroids) in severe autoimmune cases. | No cure; management is supportive: behavioral therapy (ABA, speech therapy), educational support, and medications for comorbid symptoms if needed. Dietary or biomedical interventions (like GFCF diet or supplements) are experimental – some children try folinic acid or other supplements, but responses are variable unless an underlying deficiency is identified. |
Summary: There is overlap between CFTD and autism (a child with CFTD often meets criteria for ASD due to communication and social deficits), but CFTD includes additional neurological abnormalities and has a specific cause. Crucially, identifying CFTD in a “non-verbal autistic” child is important because it opens the door to effective treatment (folinic acid), whereas idiopathic autism requires a different support approach. In practice, any child with autism who has unusual features (early regression with seizures, or a strong family history of autoimmunity, etc.) might be screened for folate issues (e.g. an FRα antibody blood test) to rule out a CFTD component.
3. Diagnostic Workup: Distinguishing CFTD from Autism and Determining Folinic Acid Need
Diagnosing autism itself is a clinical process. It involves behavioral assessments by specialists – for example, using tools like the Autism Diagnostic Observation Schedule (ADOS) and detailed history (per DSM-5 criteria). No blood test or brain scan can confirm autism; however, when a child presents with autism-like symptoms (especially if non-verbal), a comprehensive workup is often warranted to check for medical conditions that could either cause or exacerbate the developmental issues. Here we focus on tests for differentiating cerebral folate deficiency vs. primary autism, and for guiding folinic acid therapy decisions:
- Developmental and Behavioral Evaluation: First and foremost, a thorough developmental assessment is done by a pediatric neurologist or developmental pediatrician. Standardized tests will gauge the child’s cognitive level, receptive and expressive language, and adaptive skills. Autism is diagnosed by identifying the characteristic pattern of social-communication deficits and repetitive behaviors. Even if autism is diagnosed, this evaluation also notes any red flags that point to metabolic disorders: e.g. loss of skills (regression), motor signs, unusual tone or reflexes on neuro exam. Such findings would prompt further medical testing.
- Genetic Testing: It is standard of care now that children with ASD undergo genetic testing to look for etiologies. A chromosomal microarray can detect copy number variations (deletions/duplications) associated with autism. If that’s negative, whole-exome sequencing may identify single-gene disorders (for example, mutations in MECP2 for Rett syndrome, or FMR1 for Fragile X, etc.). While this doesn’t directly indicate folinic acid need, it can reveal alternate diagnoses. Notably, Rett syndrome and certain mitochondrial disorders can present with autism features and also have low CSF folate, so identifying those is important (Rett syndrome children, for instance, often have secondary CFD and might benefit from folate supplementation).
- Workup for Cerebral Folate Deficiency: If CFTD is suspected, lumbar puncture with measurement of 5-MTHF in CSF is the definitive diagnostic test. This is an invasive procedure, usually done under sedation in young children, and performed at tertiary centers. A low CSF folate confirms cerebral folate deficiency. However, lumbar puncture is not done routinely in every non-verbal child due to its invasiveness. Instead, a less invasive screening test is the Folate Receptor Antibody Test (FRAT) – a serum blood test that measures autoantibodies against the FRα. A high level of blocking FRα antibodies in a child with autism strongly suggests an autoimmune CFD is contributing. This test can be ordered through specialty labs and is often covered in research studies. A positive result indicates the child may benefit from folinic acid treatment, as documented in studies where children with FRAA responded well to leucovorin. In fact, researchers have proposed using FRAA as a biomarker to predict folinic acid responders so that one might avoid the need for lumbar puncture. In practice, if a child with ASD is FRAA-positive, many clinicians will go ahead and initiate a trial of folinic acid (while also possibly recommending removal of dairy to reduce antibody production, see section 6).
- Additional Lab Tests: Some other tests might be done to provide a broad picture or rule out other metabolic issues:
- Serum folate and B12 levels: Typically normal in CFTD (because the issue is in CSF, not blood), but it’s good to ensure the child isn’t generally deficient due to malnutrition or malabsorption. Also, B12 is another methylation cofactor; occasionally B12 deficiency can mimic developmental regression (and B12 shots along with folinic acid are another treatment approach some use for autism).
- Homocysteine and Methylmalonic Acid: These are functional markers of B-vitamin status. In pure CFTD, homocysteine might be normal or slightly elevated (if methionine synthase in brain is impaired) – though not a sensitive indicator. These tests are more to check for systemic folate/B12 metabolic disorders.
- Thyroid function and lead levels: Not directly related to folate, but part of many “speech delay” workups to exclude hypothyroidism or lead poisoning as causes of developmental delay or autistic-like symptoms.
- EEG (electroencephalogram): If a child has staring spells or regression, an EEG is done to check for subclinical seizures (like an epileptic encephalopathy). This is relevant because infantile CFD often presents with seizures that can contribute to loss of skills. If EEG shows epileptic activity, it needs treating alongside any folate issues. (Some CFD cases have a specific high-voltage slowing on EEG that improves with folinic acid.)
- Neuroimaging (MRI brain): An MRI might be performed especially if there are neurological signs. In idiopathic autism, MRI is usually normal; in CFTD, the MRI may show delayed myelination or mild cerebral atrophy in some cases. It’s not diagnostic, but if MRI shows unexplained changes (e.g. demyelination) one might consider a neurometabolic disorder like CFD.
- Deciding on a Folinic Acid Trial: Ultimately, whether to trial folinic acid can be based on the above test results combined with clinical judgment. Clear indications for a therapeutic trial of folinic acid in a non-verbal child would include:
- Positive FRα autoantibody test (especially high titers of blocking antibody).
- Documented low CSF folate (if lumbar puncture was done).
- A history of unexplained regression or neurological symptoms alongside autism (even if testing is inconclusive, a trial might be justified given folinic acid’s low risk).
- A sibling or family history of folate-related disorders. (For instance, if an older sibling with autism responded to folinic acid, one might test the younger sibling as well.)
- Note: A folinic acid trial is generally considered safe (see section 4), so some clinicians will proceed empirically for 3–6 months to see if the child improves, even in the absence of confirmatory tests, especially if access to testing is limited. If the child shows clear gains (new words, better attention) on folinic acid, that itself can validate the decision.
In summary, diagnosing CFTD vs autism often means adding a medical lens to the autism workup. Autism diagnosis will answer “does the child meet criteria for ASD?”; the medical workup answers “why is this child autistic/non-verbal?” and “are there treatable contributors like folate deficiency?”. A comprehensive approach uses both behavioral assessments and strategic laboratory tests (like FRAA, CSF studies) to uncover those children who could significantly benefit from folinic acid and related interventions.
4. Folinic Acid Treatment: Formulations, Safety, and Timeline of Response
Form of Folate – Folinic Acid vs Others: The form of folate given to children in these contexts is folinic acid, also known as leucovorin (typically provided as calcium folinate). Folinic acid is a reduced folate, one metabolic step downstream from folic acid, and does not require the dihydrofolate reductase enzyme for activation. This is important because many humans (especially young children) have limited capacity to convert synthetic folic acid to active folate in the body. Folinic acid is readily converted to 5-MTHF, the form that the brain uses. In contrast, folic acid (the common supplement form of B9) in high doses can accumulate unmetabolized and may actually compete with natural folates for transport into the brain. Therefore, simply giving large amounts of folic acid is not as effective – and could even be counterproductive – in children with folate transport issues. Folinic acid bypasses this problem by efficiently raising active folate levels in the bloodstream and CSF. Another form, 5-MTHF (L-methylfolate), is available as a supplement and can cross the blood–brain barrier. Some clinicians use high-dose methylfolate in older children or adults with folate-related disorders. However, in young children under 5, high-dose methylfolate has not been as well studied as folinic acid. Additionally, if FRα antibodies are present, 5-MTHF might still be partially blocked from entry (since FRα would bind any folate form). Folinic acid has the advantage of leveraging the RFC pathway to force folate into the brain. For these reasons, leucovorin (folinic acid) is the most effective and evidence-backed form for pediatric use in autism/CFD contexts. It’s available by prescription (historically used as a rescue agent in chemotherapy or for antifolate drug overdoses).
Dosage and Administration: In research studies, the typical dose is around 2 mg per kg body weight per day, up to a maximum of 50 mg per day, split into two doses. For a child under 5, this usually ends up being in the 20–25 mg per day range. It can be given orally (tablets or compounded into a flavored suspension). Folinic acid is well-absorbed orally; intramuscular or intravenous routes are generally not needed for chronic therapy, only for acute rescue (and those forms are used in hospitals, not home). There are both racemic folinic acid (a mix of active and inactive isomer) and levo-folinic acid (pure active isomer, sometimes called calcium levofolinate) – but in practice, the racemic leucovorin is commonly used and has shown efficacy. Importantly, when starting folinic acid, clinicians often also ensure adequate co-factors: e.g. vitamin B12 and B6 levels should be sufficient (since folate, B12, B6 work in concert in homocysteine metabolism). Sometimes B12 injections are given alongside folinic acid in autism protocols, though the primary evidence for speech improvement is with folinic acid alone.
Safety in Young Children: High-dose folinic acid is generally very well tolerated in children, including those under 5. Unlike folic acid, folinic acid is unlikely to mask B12 deficiency at these doses because it is directly utilized by cells. The main side effects observed have been mild and temporary. In clinical trials for autism, there were no serious adverse events attributable to folinic acid. A subset of children (especially those who respond behaviorally) can become temporarily more hyperactive or restless in the first few weeks of treatment. Parents sometimes report increased energy, silliness, or difficulty falling asleep when starting the vitamin – this is thought to be analogous to what is seen when starting other B vitamins or even stimulants, and it usually subsides within a month or so. If it’s troublesome, doctors might halve the dose for a short period and then build back up. In extremely rare cases, folinic acid could theoretically lower the seizure threshold (because B9 in large doses can affect neurotransmitter turnover), but in the Arkansas trial of 48 children, folinic acid recipients did not have more seizures than placebo. In fact, separate reports in CFD syndrome (where seizures are part of the condition) show seizures improve on folinic acid over time. Overall, folinic acid is considered safe for long-term use in children; it’s a bioactive vitamin, not a foreign pharmaceutical. Nonetheless, ongoing monitoring is recommended – at follow-up visits, doctors will check progress and ensure no adverse effects like irritability, rash, or gastrointestinal upset (all of which are uncommon).
One precaution is that if a child has pernicious anemia or leukemia, folinic acid should be used under guidance because it can interact with those disease processes (e.g. feeding hematopoiesis or counteracting certain chemotherapy). For the typical scenario of a non-verbal 3-year-old, these are not concerns. Also, if a child is already on antiepileptic drugs like phenobarbital or phenytoin, folate supplements can increase the metabolism of those drugs and slightly lower their levels, so coordination with a neurologist is wise for children with epilepsy.
How Long to See Results: Folinic acid is not an overnight cure; it generally takes several weeks to months to observe significant changes in speech or behavior. In the double-blind trial, by 12 weeks (3 months) the treatment group showed clear improvements in verbal communication compared to placebo. Some improvements (like increased attention span or new syllables) have been noted as early as 4–8 weeks in clinical practice. There are anecdotal reports of very fast responses – for instance, parents in one case noted their son spoke his first words after just 3 days on leucovorin – but such rapid turnarounds are not the norm. More commonly, parents and therapists report gradual progress: maybe the child starts vocalizing more or gains a few new words after a month, then gradually strings two-word phrases after 3–4 months. The typical course is to continue folinic acid for at least 6 months if any positive changes are seen by 3 months. If absolutely no change is observed in 6 months, some clinicians might discontinue it; however, given folinic acid’s safety, others might still continue if the child has FRα antibodies (on the rationale that it’s preventing further folate deficit in the brain).
For children with confirmed CFTD (e.g. FOLR1 mutation), folinic acid is a lifelong therapy – symptoms return if the vitamin is stopped. For children with autism and FRAA, the optimal duration is not fully established, but many stay on it for years during their key developmental period. It’s worth noting that improvements on folinic acid can be subtle or indirect: a child might become more alert and thus engage better in speech therapy, leading to more words – one has to gauge the overall developmental trajectory rather than expecting a single dramatic milestone.
Most Effective Use in Under-5s: The question specifically mentions children under age 5. This is a critical window for speech development (neuroplasticity is high). Folinic acid appears most effective when started early – one study noted that treating before age 6 yielded better outcomes in CFD than starting later. Thus, identifying and treating a folate issue by age 3–5 is ideal. In practical terms for a toddler: one would give leucovorin daily (often mixing a crushed tablet or solution in juice if the child won’t take pills), and monitor developmental progress. Often a developmental pediatrician or neurologist will formally reassess language after 3–6 months to quantify any changes. Families are counseled to continue all usual therapies (speech therapy, behavioral therapy) during this time; folinic acid is a facilitator, not a replacement for skill-building therapies.
Adjunct Measures: Many protocols for children with folate autoimmunity include a dairy-free diet along with folinic acid. The reason is that cow’s milk contains a folate-binding protein very similar to human FRα; in some children, consuming dairy can perpetuate the production of FRα antibodies. By removing dairy, the antibody titers may decrease over time, enhancing folinic acid’s effectiveness at reaching the brain. Some severe cases of FRAA-associated CFD have even been treated with immunotherapy (like low-dose prednisone) to reduce antibody levels, but this is usually reserved for cases with refractory symptoms. For the average young child, folinic acid (often alongside a multivitamin and Omega-3s, etc.) plus diet changes is the approach.
In summary, leucovorin (folinic acid) is the form of choice for treating folate-related speech delays. It is safe for young children and typically yields improvements within 2–3 months in those who have an underlying folate transport issue. Early and sustained treatment can significantly alter a child’s developmental course, helping non-verbal children make strides in communication that might not have been possible otherwise.
5. Gut Microbes in Autism: Overgrowth, Neurological Impact, and Interventions
The interplay between the gut microbiome and the brain (the gut–brain axis) has become a major area of autism research. Many non-verbal or autistic children have gastrointestinal (GI) abnormalities – ranging from chronic diarrhea or constipation to bloating and food intolerances – and a growing body of evidence suggests that gut microbes can influence neurological function and behavior. Here, we examine how microbial overgrowths such as Clostridia and Candida can affect a child’s neurological status and speech, and discuss interventions like diets and “detox” protocols aimed at the gut.
Gut Dysbiosis in Autism: Studies have consistently found that the gut flora of children with ASD differs from that of neurotypical peers. For example, certain bacterial groups (like Clostridia species, Desulfovibrio, and others) tend to be overrepresented in ASD, while beneficial microbes may be reduced. These microbial imbalances can lead to excess production of metabolites that act on the nervous system. Children with autism and GI issues often show more severe ASD symptoms, indicating that gut problems might aggravate neurological function. Two specific culprits frequently mentioned are Clostridium bacteria and Candida yeast.
Clostridial Overgrowth and Behavior:
Several Clostridium species (anaerobic spore-forming bacteria) have been implicated in autism. They produce short-chain fatty acids (SCFAs) and other chemicals that can affect the brain. One SCFA, propionic acid (PPA), is of particular interest. PPA is a metabolic byproduct of Clostridia and some other gut bacteria (Bacteroidetes), and it can cross the blood–brain barrier. In rodent models, intraventricular infusion of propionic acid causes neuroinflammation and behaviors reminiscent of autism (such as hyperactivity, repetitive movements, and social impairments). This suggests that high levels of PPA from gut bacteria might contribute to ASD symptoms in humans. Supporting this, some children with ASD have unusually high concentrations of Clostridia in their stools, and their urine can contain elevated levels of certain Clostridial metabolites. One such metabolite is 3-(3-hydroxyphenyl)-3-hydroxypropionic acid (HPHPA), which is produced by Clostridium species; high urinary HPHPA has been correlated with more severe behavior problems in autism in small studies. Reducing Clostridia has been shown to alleviate some symptoms: a classic example is the Sandler et al. (2000) study where 11 children with regressive autism and chronic diarrhea were given oral vancomycin (an antibiotic targeting anaerobes like Clostridia). During the 8-week course, most children showed notable improvement in communication and behavior, as documented by blinded evaluations. However, these gains faded after the antibiotic was stopped (presumably because the pathogenic bacteria grew back). This transient improvement strongly indicates a gut bacterial influence on autism symptoms. Additionally, systematic reviews have noted that Clostridium species (e.g., C. perfringens, C. histolyticum) are found at higher rates in ASD fecal samples, and their presence is associated with GI problems in these children. The take-home point is that Clostridial overgrowth can release neuroactive toxins (like PPA) that may worsen autistic behaviors and possibly impede language by affecting brain circuits.
Candida Overgrowth and Neurological Effects:
In parallel to bacteria, yeast overgrowth, especially Candida albicans, is frequently discussed in autism. Candida is a fungus normally present in the gut in small amounts, but antibiotic use, high sugar diets, or immune dysfunction can lead to overgrowth. Some children with autism have a history of repeated antibiotic courses (e.g., for ear infections), which can kill competing bacteria and allow yeast to proliferate. Candida produces metabolites such as D-arabinitol (a sugar alcohol) and potentially toxins like acetaldehyde (from fermenting carbohydrates). These can have systemic effects. Research has shown that urinary levels of D-arabinitol are often elevated in autistic children, implying significant Candida activity. One study demonstrated that giving a probiotic (beneficial bacteria) to ASD children reduced their urinary D-arabinitol levels and led to improvements in their ability to concentrate and follow instructions. This suggests that reducing Candida load can positively influence behavior and possibly cognitive function. Moreover, a study by Kantarcioglu et al. found Candida species in Yeast Overgrowth is a medical issue common to autism. পexcess: over 75% of ASD children in their sample had Candida present in stool, versus ~20% of controls. The Candida in ASD children was often in its aggressive, hyphal form, which can penetrate the gut lining. How might Candida affect speech or neurological function? There are a few theories: (1) Toxin production – Candida can produce alcohols and aldehydes that circulate to the brain, potentially causing “brain fog,” attention issues, and irritability (one might analogize it to a mild, chronic intoxication slowing cognitive processes). This could obviously impair a child’s ability to learn and use language. (2) Nutrient malabsorption – heavy yeast overgrowth can inflame the gut and impair absorption of nutrients like zinc, magnesium, B-vitamins, which are important for neural function. (3) Immune activation – a chronic Candida infection might continuously activate the immune system, leading to inflammation that affects the brain (some ASD kids have elevated cytokines that could originate from gut immune responses). Parents and clinicians have noted that treating yeast (with antifungals and diet) sometimes results in children being more present, calm, and communicative.
Neurological and Speech Impact:
Both bacterial and yeast overgrowths can exacerbate behaviors that interfere with speech development. A child with abdominal pain, bloating, or toxic metabolites from dysbiosis may be more irritable, have trouble sleeping, and have difficulty focusing on learning to speak or attending therapy. There is also speculation that certain microbial metabolites might specifically interfere with language centers in the brain or the dopamine pathways involved in motivation to communicate. While research is still nascent, one clinical insight is that when a child’s chronic GI issues are resolved, often their behavior and readiness to learn improve. For example, a toddler who used to scream and tantrum from gut discomfort might become calmer and start paying more attention to people’s speech once their belly feels better – which naturally creates better conditions for speech development. Additionally, gut bacteria can influence the synthesis of neurotransmitters; some gut microbes produce GABA, others modulate serotonin levels in the gut (which can affect serotonin in the brain). Imbalances could theoretically skew the excitatory/inhibitory balance in the brain, affecting sensory processing and language.
Protocols for Intervention: Given this connection, a number of biomedical interventions targeting the gut have been employed for autism:
- “Detoxification” (Microbial): In this context, detox often means reducing the load of harmful microbial metabolites. Approaches include:
- Antibiotics/Antifungals: Carefully chosen antimicrobial therapy can reduce pathogenic flora. Oral vancomycin (for Clostridia) as in the Sandler study is one example, though not a long-term solution. For Candida, antifungal medications like Nystatin (non-absorbed, stays in gut) or Fluconazole (systemic, for tougher cases) are used. These should ideally be guided by stool test results and done under medical supervision.
- Die-off management: When killing microbes, there can be a Herxheimer reaction (release of toxins causing transient worsening). To “detox” during this, some protocols use charcoal or clay to bind toxins in the gut, epsom salt baths to support sulfate conjugation (for toxin breakdown), and liver support supplements (like milk thistle or glutathione).
- Supporting excretion: Ensuring the child isn’t constipated is key – regular bowel movements help flush out endotoxins. Some children are given soluble fiber or probiotics to help with this after initial microbial clear-out.
- Probiotics: After reducing the “bad” microbes, high-dose probiotics are introduced to repopulate the gut with beneficial bacteria. For Clostridia issues, probiotic strains like Bifidobacterium longum and Lactobacillus rhamnosus can be helpful (they produce acids that suppress Clostridia). For Candida, probiotics plus perhaps yeast-specific enzymes can prevent regrowth.
- Dietary Changes – GAPS/SCD: Diet is a cornerstone of managing dysbiosis. The Specific Carbohydrate Diet (SCD) and the derived Gut And Psychology Syndrome (GAPS) diet both aim to eliminate foods that feed pathogenic microbes and heal the gut lining. They remove all grains, sugars (except monosaccharides like honey in moderation), many starches, and often dairy (especially in early phases). The diet instead focuses on meat, fish, eggs, vegetables, nuts, and fermented foods (yogurt in SCD, though GAPS might delay dairy introduction). The idea is that complex carbs and disaccharides that aren’t fully absorbed become fodder for Clostridia and yeasts; by removing them, one starves out the overgrowth. There is anecdotal and some clinical support for these diets: one case series found that implementing SCD/GAPS in autistic children improved their gastrointestinal symptoms and some behavioral measures without nutritional detriment. Many parents report that on diets like GAPS, their children’s diarrhea or severe constipation resolves, their eczema clears (a sign of reduced inflammation), and they seem more cognitively present. As speech is often one of the last skills to come in these children, a period of improved overall well-being and reduced gut inflammation can precede a burst of language. In younger kids, sometimes an improvement in eye contact and engagement (after diet change) leads quickly to new word usage or better responsiveness in speech therapy. It’s important to note that these diets can be restrictive; working with a nutritionist ensures the child still gets adequate nutrients (especially fiber, calcium, and vitamins).
- Other diets and supplements: Besides GAPS/SCD, some families try the Specific Carbohydrate Diet plus Low Oxalate (since certain gut bacteria overgrowths produce oxalates that can affect behavior) or Ketogenic diets(which have shown benefits for some ASD symptoms in small studies, possibly by altering gut flora and providing alternative fuel to the brain). Additionally, supplements like omega-3 fatty acids and digestive enzymes are often added. Digestive enzymes (e.g. DPP-IV enzymes) can help break down food more completely, leaving less for harmful microbes to ferment, and possibly reduce peptide absorption (related to gluten/casein issues discussed later).
- Fecal Microbiota Transplantation (FMT): A breakthrough approach in recent years has been to directly reset the gut microbiome via FMT, also known as microbiota transfer therapy. In FMT, a processed stool from a healthy donor is introduced into the patient’s gut (either orally via capsules or via colonoscopy/enema), with the aim of engrafting a healthy microbial community. An open-label trial in Arizona (Kang et al., 2017) in children with autism showed remarkable results: not only did GI symptoms improve, but autism core symptoms (language, social interaction, repetitive behaviors) improved by about 45% at a two-year follow-up. Parents reported steady gains in language and social engagement long after the FMT was done, suggesting a durable shift in the gut-brain axis. While this is still experimental, it underlines how crucial the gut microbiome is – modifying it can literally alter brain function in a sustained way. At least one child in that study went from severely autistic to mildly autistic range in evaluations two years post-FMT. For non-verbal children, such interventions have the tantalizing possibility of jump-starting development if indeed gut dysbiosis was a major holding-back factor.
- Testing the Microbiome: To tailor gut-related treatments, clinicians often use specialized tests:
- A Comprehensive Stool Analysis (with culture, microscopy, and DNA/PCR analysis) can identify specific bacterial and yeast populations and whether there is overgrowth. It can also assess markers like calprotectin (gut inflammation), short-chain fatty acid levels, and digestion markers. For instance, finding high levels of Clostridium or an overgrowth of Candida in the stool would guide targeted therapy (antibiotic or antifungal choice).
- Urinary Organic Acids Tests (OAT): These tests measure metabolic byproducts in urine that give clues about gut flora. We mentioned HPHPA (Clostridial marker) and D-arabinitol (Candida marker); an OAT can quantify these. A high HPHPA, for example, is often interpreted as a sign of Clostridia excess contributing to neurobehavioral issues. Some OAT profiles of ASD kids also show high arabinose (another possible yeast byproduct, though arabinose can be dietary too) and other unusual phenyl acids linked to bacterial metabolism. These tests, while considered “functional medicine” tools, have been used in published research to distinguish subtypes of autism based on metabolism.
- Blood tests for immune response to microbes: Some researchers measure antibodies to gut bacteria (like anti-LPS or anti-Saccharomyces cerevisiae antibodies) to see if the immune system is reacting to translocated microbes or yeast. Elevated levels might indicate a leaky gut with microbial components entering the bloodstream, which often correlates with behavioral severity.
- Clinical monitoring: Even without fancy tests, basic clinical monitoring of the child’s GI function is key. Are they stooling daily and of normal consistency? Do they have excessive gas or foul stool odor (which could imply dysbiosis)? Does the child dig at their belly or experience night waking with pain (potential signs of gut discomfort)? These observations help guide how aggressive to be with interventions. Often a therapeutic trial (diet change, probiotics) is both treatment and diagnostic – if the child improves notably, it implicates the gut in their condition.
In conclusion, gut microbial imbalances like Clostridia and Candida overgrowth can produce toxins and inflammation that impede neurological function and possibly speech development. Addressing the gut through diets (like GAPS/SCD), antimicrobial treatments, and microbiome-focused therapies can lead to better cognitive clarity and reductions in autistic behaviors. While not every non-verbal child has severe dysbiosis, a substantial subset do, and they may experience meaningful gains (sometimes even starting to speak) when their gut health is restored. This is why an integrative approach to a non-verbal child with autism often includes a GI evaluation and appropriate interventions as an essential component.
6. Food Sensitivities (Gluten and Casein) and Their Connection to Speech/Autism Symptoms
Dietary proteins – especially gluten (from wheat and related grains) and casein (from dairy) – have been suspected to affect certain children’s behavior and development. Many parents of autistic or speech-delayed children try gluten-free and casein-free (GFCF) diets and report improvements in eye contact, attention, and speech. Here we explore the scientific rationale behind these observations, and what tests can detect such sensitivities in a young child (~3 years old).
Gluten/Casein and the Opioid Theory: One long-standing theory is that some children have an inability to fully break down gluten (from wheat, barley, rye) and casein (the main protein in milk). Partially digested fragments – gliadorphinfrom gluten and beta-casomorphin from casein – can have opioid-like activity in the brain. Normally these peptides wouldn’t penetrate the gut in significant amounts, but if a child has a “leaky gut” (increased intestinal permeability), these molecules could enter the bloodstream and cross into the brain. There, they might bind to opioid receptors, causing effects like diminished pain sensitivity, lethargy or fogginess, and self-stimulatory behaviors. An analogy is being on a constant small dose of morphine – one might be detached and less responsive socially. This could obviously interfere with language learning (since the child may be in an inattentive haze). Some studies in the late 1990s and early 2000s found elevated levels of these opioid peptides in the urine of children with autism, supporting this theory, though more recent attempts have given mixed results. Nonetheless, the hypothesis explains why removing gluten and dairy (thus removing the source of those peptides) might improve alertness and responsiveness.
Immune-Mediated Food Reactions: Beyond the opioid concept, there’s evidence that many children with ASD have abnormal immune responses to gluten and casein. Research has shown a higher prevalence of antibodies against gluten and casein in children with autism compared to typical children. For instance, one study found significantly higher levels of IgG antibodies to gliadin (a gluten component) and to casein in the ASD group. These are not the same antibodies as in celiac disease or classic allergy – they indicate a possible IgG-mediated sensitivity or chronic food-induced inflammation. The presence of these antibodies suggests that gluten/casein might be triggering the immune system, leading to systemic inflammation or direct autoimmune effects that could affect the brain. In some autistic children, for example, ingestion of dairy can precipitate behavioral changes (irritability, hyperactivity) within days, which might be due to an immune reaction. Over the long term, such immune activation could exacerbate neuroinflammation, a phenomenon noted in postmortem studies of autistic brains. In a child without autism, similar mechanisms are seen in conditions like gluten ataxia – a non-celiac autoimmune reaction to gluten that causes neurological symptoms including gait disturbance and speech difficulties (dysarthria). That is a stark example of how a food protein can affect the brain.
Symptoms Tied to Gluten/Casein Sensitivity: How would a parent know if gluten or dairy might be affecting their child’s speech or behavior? Some clues include:
- The child has chronic loose stools or constipation, especially foul-smelling stools (could hint at gluten intolerance or underlying celiac).
- The child has red cheeks or ears, or blotchy skin, after consuming these foods (some parents note “behavioral allergic” signs like face flushing).
- The child’s behavior worsens notably after meals containing wheat or dairy – for instance, more hyper or “zoned out” 30–60 minutes after a cupcake or a glass of milk.
- There is a family history of celiac disease, gluten sensitivity, or dairy intolerance (these tendencies can run in families).
- The child had excessive milk drinking (beyond age 1–2) and is a “milk addict” or “bread/cracker addict.” Sometimes, kids crave the very foods they’re sensitive to, possibly for the mild opiate effect.
While these are anecdotal clues, they often prompt a trial of a GFCF diet. Many reports (and some studies) indicate that a subset of children do improve on such diets: improvements can range from better GI function and fewer tantrums to increased language output. For example, one parental survey study found that a GFCF diet led to improvements in behavior and speech in a proportion of ASD children, though others didn’t show changes. A randomized trial by Hyman et al. (2016) did not find overall group differences on the diet, but importantly, children who had gastrointestinal symptoms or signs of sensitivity tended to improve more – suggesting the diet helps those who truly have the sensitivity, but not those who don’t. So the challenge is identifying which children have the sensitivity.
Testing for Gluten and Casein Sensitivities (around age 3):
- Celiac Disease Screening: Before attributing issues to “gluten sensitivity,” one must rule out celiac disease, which is an autoimmune condition triggered by gluten that can have both intestinal and extra-intestinal manifestations (including, rarely, developmental delay or attention issues). At age 3, celiac testing is reliable if the child has been consuming wheat regularly. The standard test is IgA anti-tissue transglutaminase (tTG) antibody, along with a total IgA level to ensure the child is not IgA-deficient (IgA deficiency would make the tTG test falsely negative). A strongly positive tTG (>> upper limit of normal) virtually confirms celiac in a pediatric patient and usually warrants an endoscopy with small bowel biopsy for definitive diagnosis. Another test, IgA (or IgG) anti-endomysial antibodies, is highly specific but often not needed if tTG is positive. Additionally, IgG anti-deamidated gliadin peptide (DGP) antibodies can be useful, especially in younger children, as they sometimes pick up celiac in kids under 3 better than tTG. If any of these are positive, the child likely has celiac disease, and a strict gluten-free diet is medically necessary (and often results in improved wellbeing and sometimes developmental catch-up once nutrients are absorbed better). It’s worth noting celiac is more common in individuals with autism than in the general population in some studies, though not dramatically so. Even if speech delay is the only symptom, testing for celiac is a prudent step, as untreated celiac can cause subtle neurological issues.
- IgE Allergy Testing: Classical food allergies (mediated by IgE antibodies) to wheat or milk usually present with acute reactions (hives, swelling, vomiting, etc.), not isolated speech delay. However, some children have atypical allergic responses that could affect behavior (for example, some evidence links cow’s milk allergy to speech delay via middle ear infections and mucus production). For completeness, a pediatric allergist can perform skin prick tests or ImmunoCAP blood tests for wheat, gluten, milk, casein, and other common food allergens. If positive for IgE, removing the food is clearly indicated. In autism, about 20–30% of kids have concurrent IgE-mediated allergies (often to peanuts, eggs, etc., not necessarily gluten/casein). A study cited in Clinical Therapeutics noted that children with autism had a higher rate of positive IgE tests to foods than their siblings (36% vs 5% in one sample), indicating atopy is more prevalent in ASD. So, an IgE panel might uncover something like a milk allergy contributing to discomfort. But if IgE tests are negative, one can’t yet conclude gluten/casein are fine – non-IgE sensitivities could still exist.
- IgG and IgA Food Sensitivity Panels: These tests, available through specialized laboratories, measure IgG (and sometimes IgA) antibodies to various food proteins. They are sometimes referred to as “food intolerance tests.” In the context of autism or speech delay, practitioners may order IgG levels to gliadin (the protein in gluten) and casein. As mentioned, researchers have found autistic kids often have higher IgG to casein/gluten – one study in Nutritional Neuroscience found elevated IgA antibodies to casein and other milk proteins in autism as well. However, interpretation is tricky: IgG could just indicate frequent exposure. Still, extremely high IgG titers might suggest the body is mounting a chronic immune response. If a 3-year-old shows, say, very high IgG to both gluten and casein, that could strengthen the case to eliminate those foods and see if things improve. It’s important to note that these tests are not considered definitive by mainstream medicine (because even healthy people can have IgG to foods they eat), but in combination with symptoms they can be supportive evidence.
- Non-Celiac Gluten Sensitivity (NCGS) Assessment: There is currently no lab test that definitively diagnoses NCGS – it’s essentially a clinical diagnosis made by excluding other causes. If celiac tests are negative and allergy tests are negative, but a child still seems to react poorly to gluten, one considers NCGS. Some experimental approaches measure antibodies to gliadin that are not the typical celiac ones (e.g. IgG anti-native gliadin), or look at markers like IL-2 or IL-8 levels after a gluten challenge, but these are research tools. Practically, the diagnosis of NCGS in a child is confirmed by an elimination-challenge trial: you remove gluten from the diet, observe improvement, then reintroduce gluten to see if symptoms return. If they do, that’s strong evidence of NCGS. This can be done cautiously around age 3 with pediatric dietitian guidance. One might also do an HLA gene test (for DQ2/DQ8); if that is negative, celiac is unlikely (though NCGS can still occur in non-DQ2/DQ8 people). The absence of an easy test means one has to rely on this kind of empirical trial.
- Casein Sensitivity Testing: Apart from IgG/IgE as mentioned, there isn’t a specific common test for “casein opioid peptides” in clinical use, except in some research labs that analyze urine for beta-casomorphin. High levels of urinary casomorphin would suggest the child isn’t fully digesting casein and is absorbing that peptide; that could bolster a decision to go casein-free. Additionally, lactose intolerance tests (breath test) are different – they check for inability to digest milk sugar, not the protein. Lactose intolerance in a 3-year-old is less likely (more common in older kids), and it causes GI symptoms, not neuro symptoms.
- Folate Receptor Autoantibodies (FRA) and Dairy: Interestingly, as touched on earlier, there’s an overlap between milk sensitivity and folate issues. Bovine milk contains a folate receptor protein that can trigger antibody formation in susceptible individuals. A child with autism who has high FRA antibodies might effectively have a “milk-induced” autoimmunity affecting their brain folate. For such children, testing positive for FRAA in blood provides a clear action item: go on a strict dairy-free diet. This not only tests the impact of dairy on behavior (since one would expect improvement if dairy was contributing to symptoms) but also helps lower the antibody titer over time, potentially improving folate transport. Some clinicians will measure FRAA in any autistic child with significant language delay and autoimmune family history, as it kills two birds with one stone – identifying a folate issue and pointing to a milk issue.
- Elimination Diet Trial: Ultimately, as with NCGS, the gold standard for detecting gluten/casein sensitivity in a young child is an elimination diet. There are no definitive laboratory biomarkers for non-celiac gluten or casein intolerance, so one must rely on the child’s clinical response. Typically, one would remove both gluten and casein simultaneously (because they often co-occur in foods and their effects can overlap) for a period of at least 1–3 months. In a 3-year-old, this requires commitment, as gluten and dairy are ubiquitous in toddler diets. Parents need to find substitutes (e.g. almond milk or specialized formulas instead of cow’s milk, gluten-free breads/pasta, etc.) to maintain nutrition. During the elimination, they track changes in the child’s behavior, sleep, stool, and development. If notable improvements occur – say the child starts speaking new words or is more engaged – that’s a strong indication of sensitivity. To be certain, a re-challenge is done: reintroduce gluten/dairy (one at a time, usually) and see if there is a clear regression or decline. Parents often dread this part if their child was doing better, but it’s important for confirmation. For example, a case might go: 3-year-old non-verbal boy goes GFCF, after 1 month he makes more eye contact and says 5 words; after 2 months he’s sleeping through the night for the first time and using ~10 words. At 3 months, his parents give him a slice of bread – two days later, he has a huge meltdown and stops using those new words. This would strongly suggest a genuine gluten sensitivity affecting his neurological function. At that point, they’d resume the diet indefinitely and consider him “gluten-sensitive.”
- Other Food Sensitivities: The question focuses on gluten and casein, but it’s worth noting that other foods can also cause issues. For instance, some children are sensitive to soy (hence many go on a GFCFSF – gluten-free, casein-free, soy-free diet). Others might react behaviorally to artificial additives or high phenolic foods (like certain fruits, which is another topic related to ADHD and possibly ASD behavior). While testing for those is even more difficult, an elimination diet can be broadened to test those once the big two (gluten, casein) are addressed.
In summary, gluten and casein sensitivities do not cause classic autism, but in susceptible children they can produce a syndrome of physical discomfort and foggy cognition that can look like or exacerbate autism and speech delay. Some non-verbal children have started speaking after going gluten/casein-free – likely those were the ones truly affected by those proteins. Testing involves a combination of ruling out celiac/allergy (via standard labs) and using specialized tests (IgG panels, etc.) for hints, but ultimately a carefully monitored diet trial remains the decisive test for sensitivities in a 3-year-old. If positive, the reward (improved developmental trajectory and comfort for the child) is well worth the effort.
7. European Medical Institutions (2025) for Comprehensive Diagnostic Evaluation
When faced with a child who is non-verbal, it can be challenging to pinpoint the cause – autism spectrum disorder, metabolic issues like CFTD, gut dysbiosis, and food intolerances can all interplay. In Europe, families have access to various medical centers that offer comprehensive diagnostic testing across these domains. Such evaluations are often multi-disciplinary, combining expertise in neurology, genetics, gastroenterology, immunology, and developmental pediatrics. Below are several notable European institutions and centers (as of 2025) known for their work in these areas:
- University Hospital Liège (Belgium) – Center for Autism & Neurometabolic Syndromes: The University Hospital of Liège houses a renowned Center of Autism within its Department of Pediatric Neurology. This is where Prof. Vincent Ramaekers and colleagues have led pioneering research on cerebral folate deficiency in autism. They offer testing for folate receptor autoantibodies and have experience performing lumbar punctures to measure CSF folate when indicated. Because of their expertise, they can distinguish idiopathic autism from CFD/CFTD and have published treatment trials (folinic acid, milk-free diet, etc. for autism with FRA autoimmunity). A child evaluated here would receive a thorough autism assessment as well as tailored metabolic work-up (including mitochondrial and folate metabolism tests). Liège can be considered a referral center in Europe for suspected cerebral folate deficiency syndromes presenting with autism or speech loss. Families from across Europe consult with Prof. Ramaekers’s team for guidance on folinic acid treatment and related interventions.
- Great Ormond Street Hospital (London, UK): GOSH is one of the world’s leading children’s hospitals and has a Neurodevelopmental Assessment Clinic that covers autism diagnostics. What sets it apart is the breadth of specialties on-site. For a child with speech delay and complex issues, GOSH can provide:
- Developmental evaluations for ASD (by experienced psychologists and developmental pediatricians).
- Neurometabolic work-up: GOSH’s metabolic medicine unit and the UCLH Neurometabolic Laboratory (affiliated with nearby University College Hospital) can conduct tests like amino acid profiles, urine organic acids, and even CSF neurotransmitters/folate if needed. They will be familiar with conditions like CFTD – in fact, the Neurometabolic Unit at UCL (National Hospital for Neurology) is known for diagnosing rare neurotransmitter disorders and could analyze a CSF sample for 5-MTHF (they collaborate with GOSH for pediatric samples).
- Gastroenterology and Allergy: GOSH has a specialist pediatric gastroenterology service. They can perform endoscopies to diagnose celiac disease or intestinal inflammation, and have dietitians to supervise elimination diets. They also have an allergy clinic that can do food allergy testing, which is useful to differentiate allergy vs intolerance.
- The hospital’s researchers are involved in microbiome studies as well, so while not routine, they might facilitate stool testing or even FMT trials if a child qualifies for a study.
- Essentially, GOSH provides a one-stop comprehensive assessment: a child suspected of autism might also get genetics testing, metabolic tests, and GI evaluation all within the same institution. This integration helps in forming a holistic picture.
- Karolinska University Hospital (Stockholm, Sweden): Sweden has a strong network for both autism research and clinical genetics/metabolism. The Karolinska Institute’s KIND (Center for Neurodevelopmental Disorders) is a research center, but clinically, Karolinska University Hospital sees many autism referrals. They can offer:
- State-of-the-art genetic diagnostics (Sweden was early in adopting clinical whole-genome sequencing for developmental disorders).
- Metabolic evaluation: The hospital’s laboratories can test for things like MTHFR gene polymorphisms, folate levels, and they have published studies on folate and methylation in neuropsychiatric disorders. While not as specialized in folate autoimmunity as Liège, Swedish hospitals can send samples abroad for FRα antibody testing if needed.
- Pediatric Neurology: Karolinska handles complex epilepsies and neurometabolic cases, so a child with regression and speech loss would likely be funneled to a neurologist who can differentiate autism vs. something like CFD or an inborn error.
- Gastroenterology: They also have pediatric GI and nutrition services. In Scandinavian countries, the awareness of gluten-related disorders is high, so testing for celiac and trying a gluten-free diet in autistic children with GI issues is often done in practice.
- Karolinska is also involved in microbiome research – for instance, some Nordic studies on probiotics in autism have contributors from Sweden. Thus, a family might get access to clinical trials or at least cutting-edge knowledge on interventions like probiotics or special diets.
- Bambino Gesù Children’s Hospital (Rome, Italy): Often called “the Vatican’s children’s hospital,” Bambino Gesù is a top pediatric center in Europe with a broad range of specialties. They have a dedicated unit for Autism Spectrum Disorders within their neuropsychiatry department, but importantly:
- They are part of the MetabERN (European Reference Network for Hereditary Metabolic Disorders), indicating their expertise in metabolic testing. The hospital’s metabolic team can investigate conditions like mitochondrial dysfunction or cerebral folate issues. If a doctor in Italy suspects CFTD, Bambino Gesù is a place that can measure 5-MTHF in CSF and guide folinic acid treatment (the Italian health system allows for off-label use of leucovorin in such cases).
- Bambino Gesù also publishes research on autism comorbidities; for example, they have studied insulin resistance in autism and conducted microbiome profiling in ASD patients. This means clinically they are aware of the gut-brain links and may incorporate investigations like glucose metabolism tests or stool analyses.
- The hospital’s immunology/allergy division can evaluate food intolerances. Italy in general has seen use of IgG food panel tests in autism (some Italian researchers, e.g., in Naples, have published on elevated casein/gluten IgG in autism). A family going to Bambino Gesù could get a formal celiac workup and also advice on an elimination diet if warranted.
- They also have therapeutic programs – if a child is found to have multiple issues (say ASD with folate autoimmunity and gut dysbiosis), the various departments can coordinate a plan (folinic acid prescription, GFCF diet with a dietitian, etc.).
- Autism Centre of Excellence, Charité – Universitätsmedizin Berlin (Germany): The Charité in Berlin is one of the largest university hospitals in Europe and has a strong child neurology and psychiatry department. While autism diagnosis/treatment in Germany is often handled by child psychiatrists and developmental therapists, the Charité and other centers (e.g. Munich LMU, Tübingen) have interdisciplinary clinics for “complex autism”:
- They will do the standard ADOS evaluations for autism, but also, Germany has a tradition of thorough medical evaluation for developmental disorders. The Charité’s neuropediatric unit can run a full “Autism etiological panel” including EEG, MRI, genetics (including array CGH, Fragile X test), and metabolic blood tests.
- For folate issues: There are labs in Germany (like Medizinisches Labor Bremen) that offer folate receptor antibody testing, often in collaboration with research initiatives. A specialist at Charité aware of the recent research could order that test. Additionally, Charité’s neurochemistry lab can measure neurotransmitters and pterins in CSF if needed (they have done so for conditions like pediatric neurotransmitter diseases).
- Gastroenterology: Berlin has pediatric GI doctors who are familiar with autism-related GI problems. They might perform endoscopies to check for intestinal inflammation sometimes reported in autistic children. Also, Germany has some of the leading celiac disease experts, so testing for gluten intolerance is straightforward.
- Allergy/Immunology: The hospital can assess for food allergies and also for general immune status (some children with autism have immunodeficiencies that could predispose them to Candida overgrowth, for example).
- Charité, being a research hub, also might be involved in innovative trials (for instance, microbiota transfer or even immune-modulating therapies for ASD).
- Besides Charité, other notable German centers include Hannover Medical School (which has an autism research unit and strong immunology department) and University of Freiburg (where research on nutrition in autism has been done).
- Specialized Private Clinics (Various Countries): In addition to public hospitals, Europe has private clinics with a biomedical focus on autism. For example:
- The “Vivere” Clinic in Kiev, Ukraine (serving Eastern Europe) offers unique diagnostic panels including the FRAT™ test for folate receptor antibodies. They combine biomedical testing with conventional therapies.
- The Autism Treatment Plus center in the UK (and similar in the Netherlands) provides comprehensive testing – they often collaborate with labs like R.E.D. Laboratories (Belgium) for FR autoantibodies and Great Plains Lab (for OAT and IgG panels). While not a traditional hospital, they guide families through gut healing diets, supplement protocols (like folinic acid, B12, etc.), and allergy testing.
- TACA (Talk About Curing Autism) and other organizations maintain lists of doctors in Europe who practice integrative medicine for autism, often working in outpatient clinics. For instance, in France, there are clinics in Paris that will do stool dysbiosis analyses and heavy metal screens in autistic kids; in Spain, some centers in Madrid and Barcelona offer combined neuropsychological and biomedical evaluations (one example: Hospital Sant Joan de Déu in Barcelona has an Autism Unit and can involve their metabolic specialists as needed).
- Families seeking a truly all-encompassing analysis sometimes travel internationally. In Europe, because distances are smaller, it’s not uncommon for, say, a family from Eastern Europe to go to Austria or Germany for an autism workup, or for a UK family to consult a specialist in France.
European Reference Networks: It’s worth noting that the EU has reference networks for rare diseases. Autism per se isn’t a rare disease, but cerebral folate deficiency and certain metabolic causes of autism are. So, clinicians in one country can liaise with experts in another via networks like MetabERN or Neurometabolic ERN. For example, if a doctor in Spain suspects cerebral folate transport deficiency, they might reach out to the team in Liège or to a center in Amsterdam or London for guidance on testing and interpretation.
Specific Tests Availability:
- The Folate Receptor Autoantibody Test (FRAT) originally was developed in the US (Dr. Quadros’s lab in New York). Now, kits are available in Europe: R.E.D. Laboratories in Belgium offers the test commercially. Many of the institutions above can send a serum sample to R.E.D. Lab and get results. Some hospitals have even established their own in-house assays in research settings. By 2025, a coordinated EU effort is underway to standardize FRAA testing (so within a few years it might become more routine).
- Advanced Microbiome Analysis: Academic centers like those in the Netherlands (e.g., Maastricht University) and in Italy (e.g., University of Bologna) have research collaborations where they do 16S rRNA sequencing of autistic children’s gut flora. If a child is part of a study, they may get a detailed microbiome report. Clinically, most will rely on comprehensive stool tests done by certified labs (several in Germany and the UK).
- Food Intolerance Testing: Labs in Europe (like GENOVA Diagnostics Europe in London, or local hospital labs) offer IgG panels for foods. While NHS or public systems may not endorse IgG testing, private sector and some progressive clinics do use them. For example, in Poland and Scandinavia, IgG testing for food intolerance has gained some acceptance among pediatric gastroenterologists for chronic GI issues.
Institutions Summary:
- Liège, Belgium (CHU Liège) – Leader in folate/autism research, can test/treat CFTD.
- London, UK (GOSH & UCLH) – Comprehensive autism and metabolic workup, cutting-edge neurometabolic lab.
- Stockholm, Sweden (Karolinska) – Advanced genetics and integrated care, awareness of gut-brain aspects.
- Rome, Italy (Bambino Gesù) – Top pediatric hospital with metabolic, GI, and autism specialists, involved in relevant research.
- Berlin, Germany (Charité) – Large center with multidisciplinary approach, capable of thorough medical evaluations and international collaborations.
- Others: Vienna (Austria) General Hospital (AKH) has a metabolic unit and autism clinic (they’ve done research on folate genetics in autism), Paris (France) Necker-Enfants Malades Hospital has renowned metabolic and neurology departments which see ASD children, etc. In the context of Europe, families have options to seek second opinions or specialized tests beyond their home country if needed.
By leveraging these centers, one can systematically differentiate between autism (to be managed with educational interventions) and medical mimics or contributors like CFTD (requiring folinic acid), microbial dysbiosis (needing dietary/antimicrobial treatment), and food intolerances (managed by diet changes). The goal is to leave no stone unturned – to identify any treatable factors that could help a non-verbal child make progress in speech and overall development. With the collaborative ethos in Europe’s medical community and the cited specialized resources, children can get a truly comprehensive evaluation that addresses all possible angles of their condition.
Autism, Related Conditions, and the Power of AI (Part 2)
Great — I’ll now put together Part 2 of your article, including:
- A comprehensive comparative table showing differences between Cerebral Folate Deficiency (CFD), Autism Spectrum Disorder (ASD), Rett syndrome, and general speech delay.
- The historical development of autism diagnosis, including who defined it, why current criteria (like repetitive behaviors) are required, and how diagnostic frameworks (DSM, ADOS) came to be.
- A deep dive into how Large Language Models (LLMs) and AI/NLP technologies can be used to:
- Analyze global autism research,
- Identify which interventions (like folinic acid) show the most promise,
- Predict personalized treatment responses, and
- Build better diagnostic frameworks using patient narratives and unstructured clinical data.
I’ll include real-world examples of how AI and LLMs are already being used in autism research and diagnosis and explain the potential future pathways for AI-enhanced personalized autism care.
I’ll let you know when it’s ready.
Autism, Related Conditions, and the Power of AI (Part 2)
Comparative Overview: ASD, Cerebral Folate Deficiency, Rett Syndrome, and Speech Delay
To clarify key differences, the table below compares Autism Spectrum Disorder (ASD) with Cerebral Folate Deficiency/Transport Deficiency (CFD/CFTD), Rett Syndrome, and General Speech Delay across multiple dimensions:
| Category | Autism Spectrum Disorder (ASD) | Cerebral Folate Deficiency / Transport Deficiency (CFD/CFTD) | Rett Syndrome | General Speech Delay |
|---|---|---|---|---|
| Etiology | Complex neurodevelopmental disorder with multifactorial causes. Results from a combination of genetic predispositions and environmental influences affecting early brain development. No single cause; hundreds of gene variants and prenatal factors (e.g. advanced parental age, certain exposures) contribute to risk. | Neurometabolic disordertypically caused by impaired folate transport into the brain. Often due to folate receptor alpha autoantibodies (FRAA)that block folate entry into the CNS. In rare cases, caused by genetic mutations (e.g. FOLR1gene) leading to folate transport deficiency. | Geneticneurodevelopmental syndrome caused by mutations in the MECP2 gene on the X chromosome. Usually sporadic (not inherited) mutations in MECP2 that disrupt neuronal gene regulation. Primarily affects girls; males with a full MECP2 mutation rarely survive infancy. | Heterogeneous causes. Often due to benign developmental variation or external factors like hearing loss or lack of language exposure. May also stem from mild developmental language disorder. Not typically linked to a distinct neurological disease; often no identifiable single cause. |
| Symptoms | Core features are persistent deficits in social communication and interaction, plus restricted, repetitive behaviors and interests(RRBs). Signs range from limited eye contact and lack of peer engagement to repetitive motions or intense fixations. Language delay or atypical language (e.g. echolalia) is common, alongside sensory sensitivities. Importantly, children with ASD do notshow significant loss of skills after initial development (no major regression in most cases). | Developmental delaysoften present in infancy. Common features include irritability, sleep disturbances, poor muscle tone/coordination, seizures, and slowed development. Without treatment, children may develop muscle weakness, ataxia, and sometimes “autistic-like” behaviors(e.g. social withdrawal or communication impairment). Some cases resemble autism in social and communication deficits, though caused by metabolic folate issues. | Early regression is the hallmark. After ~6–18 months of apparently normal development, child loses previously acquired skills(speech, purposeful hand use, mobility). Eventually, profound impairments emerge: loss of speech, near-constant stereotyped hand wringing or tapping, gait abnormalities, breathing irregularities, seizures, and severe intellectual disability. Social interaction may appear autistic-like (poor eye contact, withdrawn) during regression, but the distinctive motor and systemic features(hand movements, apnea, etc.) set Rett apart. | Isolated delay in speech/language development. Child may start talking late, have limited vocabulary or trouble forming sentences at the expected age. Communication is affected, but social engagement, play, and behavior are otherwise age-appropriate. Unlike ASD, a child with pure speech delay typically uses nonverbal communication (pointing, eye contact) normally and lacks RRBs. No loss of skills (just slower to develop speech). |
| Neurological Features | No single defining neurological finding. Many individuals have atypical brain connectivity and development – e.g. differences in how brain regions communicate. Some studies show early brain overgrowth or increased local synaptic connections (“hyper-connectivity”) in infancy, while others find long-range under-connectivity. Neurological exam can be normal. Seizures occur in a subset (~20–30%) but are not universal. Central coherence (integrating information) may be reduced, reflecting how the autistic brain processes information. Overall, ASD is neurodevelopmental but non-degenerative – skills can improve with intervention, and there is no ongoing neurodegeneration. | Low folate in the central nervous system is the key biochemical feature. Lumbar puncture shows low 5-MTHF in cerebrospinal fluiddespite normal blood folate. Neurologically, epileptic seizures are common (often beginning in infancy), and motor abnormalities like ataxia or spasticity may develop without treatment. Some infants have reduced head growth (acquired microcephaly) and white matter changes on MRI due to demyelination. Notably, providing folinic acid can prevent or reverse many neurological symptoms if started early, highlighting the metabolic nature. | Progressive neurological disorder. After regression, children often have microcephaly (head growth decelerates). Almost all have abnormal EEG activity and epilepsy at some point. Motor apraxia(difficulty planning movements) is profound – even if muscle strength is normal, purposeful hand use and coordination are severely impaired. Other features: breathing dysregulation(episodes of hyperventilation or breath-holding while awake), autonomic nervous system dysfunction (e.g. irregular heart rhythm, gut motility issues). Importantly, Rett is neurodevelopmental but also neurodegenerative in early childhood – skills are lost and neurological function declines before stabilizing in later years. | Typically normal neurological exam. No unusual neurological signs beyond speech/language. Hearing should be intact (if hearing loss is present, that is a separate cause of language delay). Brain imaging is usually normal. These children do not have abnormal motor patterns or seizures attributable to the speech delay itself. In essence, their brain development is typical except for the specific domain of language. (Clinicians will often perform a hearing test and developmental assessment to ensure there are no broader neurological issues causing the speech delay.) |
| Genetic/Metabolic Markers | No single biomarker for diagnosis. Hundreds of genes have been implicated; for example, de novo mutations or copy number variants in genes like SCN2A, ADNP, CHD8, etc., can each lead to autism in a subset. In ~15-20% of cases, a known genetic syndrome is identifiable (Fragile X, Tuberous Sclerosis, etc.), but most cases are polygenic or idiopathic. No consistent metabolic abnormalities across all ASD, though subsets show issues (e.g. some have elevated serotonin or immune markers). Genetic testing (chromosomal microarray, whole exome) is often done after an ASD diagnosis to look for etiological clues, but genetic heterogeneity is large. | Definitive lab markers: Low CSF 5-methyltetrahydrofolate (5-MTHF) is the hallmark. Serum folate receptor alpha autoantibodies (blocking type) are present in a majority of cases – one meta-analysis found ~71% of children with ASD had FRAA, highlighting a large overlap. In inherited transport deficiency (CFTD), homozygous mutations in FOLR1 (the gene for folate receptor-α) are identified via genetic testing; this is extremely rare (fewer than 20 cases reported). Mitochondrial dysfunction markers (e.g. abnormal lactate) are sometimes seen, as mitochondrial energy is needed for folate transport. Biomarker summary: FRAA in serum, low 5-MTHF in CSF, and in genetic cases, FOLR1 mutation confirmation. | MECP2 mutation in 80–97% of clinically diagnosed cases. Genetic testing of the MECP2 gene (blood DNA test) is the primary marker and will confirm diagnosis in the vast majority of girls with classic Rett. (In the remaining cases, other rare gene mutations like CDKL5or FOXG1 can cause atypical Rett-like syndromes.) There are no metabolic biomarkers; routine labs are usually normal. Thus, diagnosis is mainly by MECP2 genetic testplus the clinical picture. Notably, even if an MECP2 mutation is found, the child must meet clinical criteria for Rett to be diagnosed – the genetic result supports but doesn’t solely define the syndrome. | No specific biomarkers for an isolated speech delay. Genetic tests and metabolic panels are typically normal. (If they’re abnormal, the speech delay is likely part of a larger condition.) By definition, general speech delay is a diagnosis of exclusion – clinicians ensure there’s no autism, intellectual disability, hearing loss, or genetic syndrome. Thus, no unique blood test or gene defines a simple speech delay. It is identified through normal findings elsewhere except for delayed speech. |
| Behavioral Criteria | Diagnosis requires meeting DSM-5 criteria for ASD: deficits in social communication/interaction (e.g. lack of reciprocity, impaired nonverbal communication, difficulty developing relationships) and presence of restricted/repetitive behaviors or interests. These behaviors can include repetitive movements (hand flapping, lining up objects), insistence on sameness/routines, highly fixated interests, or sensory sensitivities. The DSM-5 mandates at least two types of RRBs alongside the social criteria – this requirement ensures the diagnosis captures the full ASD phenotype (scientifically, repetitive behaviors are considered a core feature, distinguishing ASD from pure social-communication disorders). Clinical evaluation often uses structured instruments like the Autism Diagnostic Observation Schedule (ADOS), a play-based assessment considered a gold-standard tool, and detailed caregiver interviews (e.g. ADI-R). These help standardize observation of the DSM behaviors. | No specific behavioral diagnostic criteria for CFD itself – it is identified by lab tests rather than a checklist of behaviors. Many children with CFD, however, exhibit behaviors that overlap with autism (e.g. communication delays, social disengagement, stereotypies) or with other neurological disorders (irritability, feeding problems, etc.). Some cases initially meet criteria for ASD and get an autism diagnosis, only later to find a folate issue. In general, clinicians suspect CFD in an autistic or developmentally delayed child if there are unexplained neurological symptoms (seizures, abnormal movements) or regression, especially if accompanied by irritability and insomnia in infancy. Thus, CFD’s “criteria” are more medical: evidence of low CNS folate and a symptom constellation, rather than a behavioral definition. | Clinical diagnostic criteria (established by consensus): Requires the developmental regression in early childhood plus the classic features. Essential criteria for Rett include: apparently normal development for the first 6–18 months, followed by loss of spoken language, loss of purposeful hand use, and emergence of gait abnormalities or apraxia. Additionally, stereotyped hand movements (hand wringing or clapping) must appear. These behavioral criteria differentiate Rett from autism: an autistic child typically does not lose skills so dramatically after a period of typical development. Rett also explicitly excludes cases where brain injury or another known disorder could explain the symptoms (exclusion criteria). The presence of an MECP2 mutation supports the diagnosis but the behavioral phenotype is paramount. | Developmental milestones criterion: Child’s expressive language is significantly behindage expectations. For instance, no words by 18 months, or <10 words by 2 years, etc., depending on norms. No other social or cognitive deficits of note – the child interacts, plays, and responds normally aside from speech. Because it’s not a formal DSM disorder, there isn’t a strict “behavioral checklist” beyond clinical judgment that speech (and possibly language comprehension) is delayed. Often a speech-language pathologist will evaluate and confirm that the child’s only issue is speech (perhaps mispronouncing sounds or limited vocabulary) and that non-verbal communication is used appropriately(e.g. pointing, gesturing, engaging with others). A key distinction is that repetitive behaviors or restricted interests are absent, and any social difficulties are proportional to not being able to speak (e.g. frustration tantrums) rather than a fundamental lack of social interest. |
| Response to Treatment | Early intensive behavioral interventionis the cornerstone. Therapies such as Applied Behavior Analysis (ABA), the Early Start Denver Model, speech and occupational therapy can significantly improve IQ, language and social skills when started in toddler years. Many children show gains in communication and adaptive behavior with appropriate support, though they will likely remain autistic (autism is lifelong). There is no medication that “cures” ASD, but medications are often used to manage co-occurring issues like anxiety, ADHD symptoms, or irritability (for example, ABA plus an atypical antipsychotic for severe irritability). Overall, with the right support, children with ASD can learn and develop markedly – outcomes vary from needing ongoing substantial support to living independently, depending on severity. Prognosis improves with early and personalized intervention, but core social challenges usually persist to some degree. | Dramatic improvements with the right treatment.The standard treatment is high-dose folinic acid (leucovorin) to bypass the folate transport issue. Folinic acid supplementation can markedly improve symptoms: studies show gains in language, attention, and reduction in autistic symptoms in children with ASD who were positive for folate receptor autoantibodies and treated with folinic acid. In a randomized trial, 12 weeks of high-dose folinic acid significantly improved verbal communication in autistic children with language delays – especially in those with FRAA, who showed large effect size improvements. Seizures and motor skills often improve as well if folinic acid is started early; untreated, seizures can be intractable. Other treatments: if an autoimmune basis, sometimes immunotherapy (e.g. steroids or IVIG) has been attempted in research settings. For the genetic FOLR1 cases, lifelong folinic acid is needed and can halt neurodegeneration and even partially reverse regression if begun promptly. In summary, response to folinic acid is typically positive, preventing further deterioration and improving development, making CFD one of the few developmental conditions that is highly treatable. | Supportive care, recently augmented by a targeted therapy. There is no cure for Rett, and historically treatment has been symptomatic: anticonvulsants for seizures, physical therapy for mobility, speech therapy (though most individuals remain nonverbal), and nutritional support (feeding tubes in severe cases). Interventions like occupational therapy can help with hand use and communication devices can assist nonverbal individuals. In 2023, the first disease-specific drugwas approved: trofinetide (Daybue), which showed modest improvements in Rett syndrome symptoms in clinical trials and is now FDA-approved for ages 2 and up. Trofinetide is thought to target pathways affected by MECP2 deficiency. While not a cure, it may improve communication and reduce irritability in some patients. Overall, the approach is long-term management: controlling seizures, treating breathing and orthopedic issues, and maximizing abilities with therapy. Many individuals with Rett live into middle age with ongoing care. | Often excellent with appropriate intervention. For a child with isolated speech delay, speech-language therapy is highly effective. Therapy can involve exercises to improve articulation, expand vocabulary, and encourage two-way communication. Many “late talkers” catch up to peers after months or a few years of therapy and enriched language exposure. If a specific speech sound disorder is present, targeted practice can correct it. The prognosis is generally good: most children with a pure speech delay (and no other developmental issues) will eventually develop normal speech and language, especially if the delay was mild to moderate. It’s crucial to address any underlying causes (for example, if chronic ear infections caused hearing loss, treat those). Parental involvement – reading to the child, encouraging conversation – further boosts outcomes. In summary, with early intervention, most isolated speech delays resolve or greatly improve, and the child goes on to have typical communication skills. |
| Age of Onset | Symptoms emerge in early childhood. Some subtle signs (lack of eye contact, not responding to name, limited babbling) can be seen by 12–18 months of age in many cases. However, the average age of diagnosis is around 3–4 years, partly because that’s when social and communication delays become more obvious and when evaluations typically occur. Importantly, autism is usually present from infancy – caregivers may retrospectively note that the baby was quiet, didn’t point or interact typically. Unlike degenerative conditions, ASD signs do not start after a period of normal development; developmental differences are there early, even if not recognized until toddlerhood. (Earlier signs often include delayed speech and limited social smiling.) | Infantile onset. In classic (autoimmune) CFD, babies may appear normal at birth but by 4–6 months start showing issues: irritability, poor feeding, not meeting motor milestones, etc. Symptoms can begin as late as the second year in some milder cases, but most often <12 months is when developmental derailment is first noted. If caused by maternal autoantibodies, signs can even be present in the first months of life (e.g. fussiness, slow development). For inherited FOLR1 transport deficiency, onset is typically around 4–5 months with developmental slowing or regression and seizures. Thus, earlier than typical autism. An infant who was developing normally might plateau or regress before their first birthday. By age 2–3 (when autism is usually being diagnosed), a CFD child without treatment would often have clear neurological problems (e.g. seizures, ataxia). | Clear onset in toddlerhood after an initial normal period.Development is normal for 6–18 months, as the child meets early milestones like sitting, babbling, maybe a few words. Then a regression phase occurs typically around 1 year of age (can be as early as 6 months or as late as 2 years). During this regression (Stage 2 of Rett), the child loses language and purposeful hand skills over weeks or months and social withdrawal emerges. By age 2, most girls with Rett have had noticeable regression. The diagnostic hallmark is this timing: onset in late infancy, compared to autism which is present from infancy (even if diagnosed later) and compared to speech delay which often isn’t evident until around age 2. | Typically noted in the toddler years.Many children are identified as “late talkers” around 2 years old when they have not met expected language milestones (like saying single words or simple phrases). Some milder speech delays might not be obvious until age 3, when peers are talking in sentences and the child is not. Essentially, once verbal communication is expected and is absent or limited, the delay becomes apparent. Unlike ASD or Rett, there is no early infancy sign – these children often babbled and cooed normally as babies and hit other milestones on time. It’s around the time when speech should bloom (18 months to 2 years) that it becomes clear the child is lagging. There is no regression; rather, it’s a failure to progressat the typical rate in speech. Many parents seek evaluation when their child is ~2 and not talking, which is when a general speech delay is formally recognized (after ruling out autism or hearing issues). |
| Diagnostic Tests | No definitive laboratory test for ASD – it’s diagnosed by behavioral assessments. Tools like the ADOS-2 (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview) are often used by specialists to systematically evaluate the child’s social interaction, play, communication, and behaviors. These, combined with DSM-5 criteria, form the basis of diagnosis. A developmental pediatrician or psychologist usually makes the diagnosis after observations and parent reports. Ancillary tests: Genetic testing is recommended after an ASD diagnosis to look for an underlying genetic cause (e.g. Fragile X or other syndromes), but this doesn’t confirm “autism,” it only finds causes in some cases. Likewise, hearing tests may be done to ensure hearing loss isn’t causing social unresponsiveness. Brain MRI or EEG is not routine unless there are atypical features (e.g. seizures or a developmental regression suggestive of another condition). In summary, diagnosis is clinical, using standardized behavioral criteria and instruments, not a blood test or scan. | Specialized labs required. The key diagnostic test is a lumbar puncture to measure 5-MTHF level in cerebrospinal fluid. A low value confirms cerebral folate deficiency. However, because a spinal tap is invasive, many clinicians first do a serum test for folate receptor autoantibodies (FRAA) – high levels of blocking FRAA strongly suggest CFD. If FRAA are positive, some doctors will empirically start folinic acid and see if the child improves, given the treatment is low-risk. For a definitive diagnosis, though, demonstrating the low CSF folate is ideal. In suspected transportdeficiency (genetic CFTD), genetic testing for FOLR1 mutations is done (e.g. through whole exome sequencing or a targeted gene panel). If a mutation is found in a child with the compatible syndrome, it confirms the diagnosis. Other supportive tests: MRI brain may show white matter changes (leukodystrophy) in longstanding cases; EEG might show nonspecific slowing or seizure activity. In practice, a combination of laboratory evidence (low CSF folate or positive autoantibodies) and clinical suspicion leads to the diagnosis. | Genetic testing is the gold standard. A blood DNA test for MECP2 mutationwill confirm Rett syndrome in the majority of cases. Any child (usually girl) who presents with regression and Rett-like features is referred for genetic testing. While waiting for results, clinicians use the clinical criteria to make a provisional diagnosis. In fact, formal diagnostic guidelines for Rett emphasize clinical observation (regression, hand stereotypes, etc.) as the first step. Once an MECP2 mutation is identified, it solidifies the diagnosis (assuming the phenotype fits). Additionally, doctors might do tests to manage complications: EEG for seizures, EKG for QT interval (heart) problems, and others – but those are to evaluate severity, not to diagnose Rett itself. So, the definitive “test” is the MECP2 genetic test, along with a thorough developmental history documenting the characteristic course. Notably, if a child has a MECP2 mutation but did not have a regression or doesn’t show the classic signs, clinicians might not label it Rett syndrome – they’d monitor closely instead. | Evaluation by specialists. There is no medical test for a simple speech delay. Hearing evaluationis crucial – an audiologist must confirm the child can hear properly, since undetected hearing loss can cause apparent speech delay. A speech-language pathologist administers standardized tests of language understanding and expression to quantify the delay. Often a developmental pediatrician or neurologist is consulted to ensure the child’s other developmental domains are normal (ruling out autism, intellectual disability, etc.). Screening toolslike the M-CHAT (for autism) might be used to document that autism signs are absent. If all other areas check out and only speech is behind, the diagnosis is essentially made by excluding other diagnoses. In rare cases, an MRI or blood tests might be done if the doctor suspects something neurological, but for an isolated speech delay these are usually normal. Thus, the “diagnosis” is a clinical judgment supported by normal findings elsewhere and a failed speech milestone test. |
Sources: The table integrates information from clinical research and expert guidelines, providing a side-by-side comparison for clarity.
Historical Evolution of Autism Diagnosis
Early Definitions: Kanner and Asperger
Autism as a distinct condition was first defined in the mid-20th century. In 1943, Austrian-American child psychiatrist Leo Kanner published a landmark paper describing 11 children with a unique constellation of symptoms he called “early infantile autism.” These children had profound difficulties in social engagement and communication, a desire for sameness, and repetitive behaviors. Kanner’s detailed description – highlighting traits like “autistic aloneness” and “insistence on sameness” – essentially set the clinical prototype for autism. Around the same time (1944), Viennese physician Hans Asperger described a group of boys with seemingly normal language development but marked social oddities and narrow interests (“Autistic psychopathy” in his terms). His work (in German) laid dormant in the English-speaking world for decades, but later became influential for recognizing a broader autism spectrum (what we came to know as Asperger syndrome).
In the early years, autism was extremely misunderstood. It was often conflated with childhood schizophrenia or blamed (erroneously) on parenting (the disproven “refrigerator mother” theory of the 1950s–60s). By the 1970s, research by pioneers like Lorna Wing and Michael Rutter helped establish autism as a neurodevelopmental condition present from early childhood – not a psychosis or attachment problem. Wing, in particular, introduced the idea of an autism spectrumin 1979, noting that there is a “triad of impairments” (social interaction, communication, imagination) that can vary in intensity. She and colleagues found many children who didn’t meet Kanner’s strict criteria but still had milder forms of the social and communication difficulties, coining the term “on the broader autism spectrum”. This work broadened conceptions of autism beyond Kanner’s narrow definition and paved the way for diagnostic changes.
From DSM-III to DSM-5: Changes in Diagnostic Criteria
The formal psychiatric recognition of autism came with the DSM-III (Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition) in 1980. For the first time, “Infantile Autism” was listed as a distinct disorder, under a new class of Pervasive Developmental Disorders (PDD). DSM-III criteria were fairly strict (monothetic) – all listed features had to be present for diagnosis. These included onset before 30 months, pervasive lack of responsiveness to others, gross deficits in language, peculiar speech characteristics, and ritualistic or repetitive behaviors. The inclusion of autism in DSM-III was a milestone, but clinicians soon found the criteria too rigid. Many children with “autistic features” were left out if they didn’t check every box.
By DSM-III-R (1987), the criteria were loosened to be polythetic (allowing a subset of symptoms), acknowledging the heterogeneity of autism presentations. Then DSM-IV in 1994 expanded the category by defining Autistic Disorder and adding separate diagnoses for Asperger’s Disorder, PDD-NOS (Pervasive Developmental Disorder–Not Otherwise Specified), as well as listing Rett’s Disorder and Childhood Disintegrative Disorder under the PDD umbrella. DSM-IV required impairments in three domains: social interaction, communication, and repetitive behaviors – often called the “triad” – and allowed more flexibility in meeting criteria. Importantly, the inclusion of Asperger’s gave diagnostic recognition to individuals with autism-like social deficits and restricted interests but without language delay or intellectual disability. This was influenced by translating Hans Asperger’s work into diagnostic practice, reflecting the broad spectrum concept.
Research in the 1990s–2000s continued to show that the distinctions between Autistic Disorder, Asperger’s, and PDD-NOS were not very consistently applied – they were often arbitrary and clinicians across centers didn’t agree who was “Asperger” vs “autistic.” By the late 2000s, consensus grew that autism is best seen as a single spectrum with individualized symptom severity. This led to a major change in DSM-5, released in 2013. DSM-5 collapsed all the sub-diagnoses into one unified Autism Spectrum Disorder (ASD) diagnosis. It also streamlined the core domains from three to two: (1) social communication deficits and (2) restricted/repetitive behaviors, since it was recognized that social and communication deficits overlap and co-occur. The DSM-5 requires evidence of both domains. It also relaxed the age of onset criterion – instead of “symptoms before age 3,” it says symptoms must emerge in the early developmental period, but may not be fully manifest until social demands exceed capacity (allowing for later recognition in some cases). This accommodates situations like very bright autistic individuals whose issues become obvious only later in childhood.
One notable scientific rationale in DSM-5 was requiring at least one type of repetitive/restricted behavior for an ASD diagnosis. This was based on research and clinical observation that while some individuals (previously diagnosed with PDD-NOS) had social communication difficulties without any RRBs, those cases often differed from true autism – for example, they might be more accurately termed Social (Pragmatic) Communication Disorder if no RRBs are present. The repetitive behaviors (which can include sensory abnormalities) seem to reflect underlying neurological features of autism, such as atypical sensory processing or need for predictability. Requiring RRBs thus increases diagnostic specificity – it helps distinguish ASD from other social/communication disorders. In fact, long before DSM-5, clinicians like Kanner and Wing noted that insistence on sameness and stereotyped behaviors were a core part of autism. Modern research also indicates that these behaviors have biological underpinnings (e.g. differences in neural networks related to habit formation and sensory gating). So the DSM-5 criterion ensures that an “autism” diagnosis captures both social–communication impairment and these characteristic behaviors, aligning with the intuitive clinical picture. (Notably, DSM-5 also added sensory sensitivities into the RRB domain, recognizing they are common in ASD.)
In summary, over time the diagnostic concept swung from very narrow (DSM-III’s rigid criteria) to broader (DSM-IV’s spectrum of PDD subtypes) and then to a unified spectrum with clearer requirements (DSM-5). This evolution was guided by research evidence and the need for both sensitivity and specificity in diagnosis. Today, “ASD” encapsulates everything from a nonverbal child with classic Kanner autism to a verbally fluent adult with subtle social challenges, differentiated by specifiers (e.g. with/without intellectual impairment) or severity levels rather than separate diagnoses.
The Rise of Standardized Diagnostic Tools (ADOS, ADI, etc.)
Alongside the formal criteria, diagnostic tools were developed to improve reliability. The Autism Diagnostic Observation Schedule (ADOS), first introduced in the 1980s and now in its 2nd edition, became a gold-standard instrument for observing the social and communicative behavior of individuals suspected of autism. During an ADOS, a trained examiner engages the child or adult in a semi-structured play or conversation session, creating opportunities for social interaction, communication, and imaginative use of objects. The clinician then codes behaviors (eye contact, sharing of enjoyment, gestures, unusual sensory interests, etc.) to see if they meet cutoffs for ASD. Because autism can present differently at different ages and language levels, the ADOS has modules (toddler, nonverbal child, verbal child, adolescent/adult) to allow standardized assessment across the spectrum.
Similarly, the Autism Diagnostic Interview–Revised (ADI-R) is a structured interview for caregivers, covering the developmental history and behaviors relevant to autism (e.g. language milestones, social reciprocity, repetitive behaviors). These tools were painstakingly validated and give clinicians a common framework. By the 2000s, most research studies required an ADOS and/or ADI-R to confirm autism in participants, which greatly increased the consistency of diagnoses in autism research.
Over time, the ADOS and ADI-R (often used together) became widely used in specialty clinics as well, to supplement clinical judgment. Their adoption helped “standardize” what criteria like DSM-IV or DSM-5 mean in practice. For example, one clinician’s interpretation of a child’s social deficits might differ from another’s; but if both use ADOS, there’s an objective scoring algorithm to decide if the child’s behaviors meet the threshold for ASD. This improved diagnostic agreement and early identification.
It’s important to note, though, that these tools are aids – the DSM criteria remain the defining requirements. In practice, an autism evaluation might involve parent questionnaires, direct observation (perhaps with the ADOS), and clinical judgment to see if DSM-5 criteria are met. Over the years, the combination of evolving criteria and tools means today’s diagnoses are more reliable and earlier than in past decades. (In the 1980s, many children weren’t diagnosed until school age; now pediatricians screen at 18 and 24 months and specialists diagnose by age 2 in many cases.)
Why Repetitive Behaviors Became Essential for Diagnosis
As touched on above, one major conceptual change was affirming that repetitive behaviors and restricted interests are a core feature of ASD, not just an accessory. Scientifically, this came from decades of observation that these behaviors co-occur with the social deficits and likely reflect the unique neurology of autism. Repetitive behaviors can range from motor mannerisms (rocking, hand-flapping) to intense special interests (memorizing train schedules, obsessively focusing on a topic) and sensory fascinations. They might seem separate from social problems, but in autism they often intertwine (for instance, difficulty with change in routine – a behavior – is related to anxiety in social situations). Research has shown that including an RRB criterion improves diagnostic validity – children with only social delays but no RRBs often have different outcomes (they may be more likely to outgrow the issues or be re-diagnosed with something else). In contrast, children who do have repetitive behaviors along with social communication deficits are much more likely to have the “full” autistic neurotype.
There’s also a neurobiological rationale: imaging studies indicate that brain circuits involved in habit formation, motor planning, and sensory processing show differences in autism, which manifest as RRBs. For example, insistence on sameness may relate to reduced adaptability in certain brain networks. By requiring evidence of these behaviors for diagnosis, the DSM-5 ensures that the diagnosis maps onto a more homogenous group in terms of underlying neural differences. Clinically, it also distinguishes ASD from conditions like Social (Pragmatic) Communication Disorder(which has social communication deficits without RRBs) or from general developmental delays where a child might have poor social skills simply due to cognitive impairment.
In short, the insistence on repetitive behaviors for an ASD diagnosis is grounded in the idea that autism is defined by a duality of social communication differences and behavioral uniqueness. Both aspects are needed to capture what autism truly is. This has helped sharpen research and treatment focus – for instance, interventions for ASD often explicitly target not just social skills and communication, but also aim to address restrictive behaviors or sensory needs.
Harnessing AI and NLP in Autism: The Potential of Large Language Models
Beyond clinical evolution, the autism field is now experiencing a wave of innovation from artificial intelligence. Large Language Models (LLMs) – AI systems like GPT-4 trained on vast amounts of text – and other Natural Language Processing (NLP) techniques are being explored for their ability to recognize patterns and generate insights from huge datasets. In 2025, researchers and clinicians are leveraging these tools in a variety of ways to advance autism understanding and care:
Analyzing Global Autism Data with NLP
The volume of autism research and clinical reports worldwide is staggering – thousands of scientific papers, case studies, and patient records. NLP can serve as a powerful “reader” that digests this global knowledge. For example, AI text-mining techniques have been used to trawl through biomedical literature and extract mentions of autism-related genes, biomarkers, and interventions. One study identified potential new biomarker genes (such as HOXB3, NR2F2, and others) by mining hundreds of research abstracts for recurrent genetic associations with ASD. This automated literature review sifted through myriad findings and highlighted which genes appear most frequently and significantly – a task that would be exhausting manually.
LLMs, with their advanced understanding of language, can take this further by synthesizing findings across papers. Imagine feeding an LLM thousands of autism research articles – the model could potentially output a summary of “what the evidence shows” on a given question (e.g., the role of immune dysfunction in ASD), complete with nuanced details from various studies. Similarly, NLP can analyze clinical reports from around the world (with appropriate de-identification) to spot patterns. For instance, by parsing text from developmental evaluations or educational reports, an AI might detect subtle commonalities in how autism presents in different cultures or note an increase in certain phrases over time (perhaps indicating new awareness of sensory issues or co-occurring anxiety).
An emerging application is using LLMs to deconstruct clinical intuition. A recent study in Cell (2025) actually used a large language model to analyze clinician’s notes and decisions in autism diagnostics, essentially trying to mimic and interrogate the logic behind expert diagnoses. By training on detailed clinical report narratives, the AI learned to predict diagnoses and identify which textual cues (e.g. “lack of response to name” or “collects objects”) were most indicative. This kind of model can reveal which features in narrative form carry the most weight – potentially enlightening us on biases or overlooked signs. It’s like holding up a mirror to the expertise of hundreds of autism specialists, distilled by an AI.
Uncovering Patterns in Treatments and Outcomes
Another area is scanning troves of patient data to find what treatments work best for whom. Autism is notoriously heterogeneous – an intervention that helps one child may not work for another. Here, AI can help by detecting patterns across many cases. For example, researchers have begun using machine learning on electronic health records of autistic individuals to see if there are subgroups who respond well to certain therapies (like ABA, speech therapy, or medications). An LLM could comb through progress notes and extract mentions like “made notable gains in eye contact after starting intervention X” and correlate that with child profiles.
One prominent instance involves the nutrient folinic acid (leucovorin), which we’ll dive into in a case study below. There have been scattered reports and studies that high-dose folinic acid can improve communication in a subset of autistic children – particularly those with an underlying folate metabolism issue. NLP can compile these reports from various journals and conferences, even parent anecdotes in forums, to quantify the pattern. In fact, a systematic review used tools to aggregate studies on folate receptor autoantibodies and folinic acid treatment in ASD, finding that about 38% of children with ASD had evidence of cerebral folate deficiency and that folinic acid led to improvements in a significant portion of those cases. By pooling data, AI can strengthen the case that “yes, this subset tends to benefit.”
Beyond folinic acid, consider behavioral therapies: Some children in early intervention programs make huge leaps, others modest gains. Machine learning algorithms have been used to predict which children will have the best outcomes from certain therapies based on pre-treatment characteristics (like initial language level, IQ, or even gene expression profiles). These algorithms, trained on past data, essentially form decision trees or neural network models that say “if a child looks like this, they are likely to respond well to therapy A, but if they look like that, therapy B might be better.” In one study, a supervised machine learning method could predict outcomes of an exercise intervention for kids with ASD, confirming that AI can crunch complex developmental data to foresee who benefits most. In the future, an LLM might take a child’s whole clinical description (perhaps extracted from reports via NLP) and then consult a knowledge base of outcomes to suggest an optimal intervention plan.
Identifying Emerging Biomarkers and Subtypes
AI is also accelerating the discovery of biomarkers – measurable indicators of biological processes in autism. This spans genetics, metabolomics, neuroimaging, and even less obvious domains like eye movements or voice patterns. By applying machine learning to large datasets (e.g. tens of thousands of genomic sequences or metabolic profiles), researchers have identified clusters of autistic individuals with shared biomarker signatures. For example, text-mining and data analytics have pointed to certain oxidative stress and mitochondrial markers that repeatedly crop up in autism studies, hinting at biochemical subgroups. One recent bibliometric analysis used NLP to map out all the biomarker research in ASD and found key themes like immune dysregulation, gut microbiome metabolites, and neuroinflammation as recurring threads, suggesting these as important biomarker categories.
LLMs specifically can help by reading through all that biomarker literature and summarizing: “Many studies report elevated cytokine X in ASD, often linked with Y symptom.” This can guide researchers to focus on the most promising leads.
Beyond text, some AI models process other data modalities. For instance, computer vision algorithms (another branch of AI) have discovered physical or neurological biomarkers: A deep learning model recently analyzed retinal photographsof children and could distinguish those with autism from typically developing peers with striking accuracy (AUC of 1.00 in one study). It appears that subtler structural changes in the retina (perhaps reflecting early brain development differences) can be a marker – something that wasn’t known until AI unearthed it. Similarly, eye-tracking patterns have emerged as a biomarker for social attention differences in ASD. The FDA-cleared EarliPoint device (more on it later) uses AI to interpret eye-tracking data; it found that how a toddler looks at social scenes vs. non-social visuals can differentiate ASD, and even gauge severity, objectively by detecting up to 1,000 subtle “looking deviations” in a session.
By identifying these patterns, AI is essentially carving autism at its joints – suggesting that there are autism subtypesdefined by biology. For instance, one subtype may involve immune system overactivation (detected via biomarkers like certain autoantibodies), another may involve synaptic gene mutations (found via genomics), another metabolic dysfunction (via metabolomic signatures). In 2025, we’re seeing the beginnings of an AI-assisted reclassification of ASD into subgroups that may one day receive tailored treatments.
Early Detection and Screening with Language Analysis
Early diagnosis is critical for autism, and AI is pushing the boundaries of how soon and how accurately we can flag signs. Large Language Models and NLP can analyze unstructured data – like what a parent writes about their toddler, or transcripts of a young child’s speech – to detect red flags.
For example, researchers have used NLP on parental narratives (those lengthy descriptions parents often give about their child’s behavior) to see if certain words or themes predict an eventual autism diagnosis. An LLM could take a parent’s statement, “He doesn’t talk much and doesn’t respond when I call him; he’s very focused on lining up his cars,” and recognize that as a likely ASD scenario versus, say, a language delay scenario where the parent might say “He’s social and plays with us, just his words aren’t coming.” By training on large datasets of such narratives (where outcomes are known), the LLM learns the patterns that correlate with autism.
Speech and language sample analysis is another promising domain. Autistic children, even when verbal, often have distinctive language features – for instance, using unusual phrasing, echoing others (echolalia), or mixing up pronouns. A 2023 study demonstrated that ChatGPT (an LLM) can be leveraged to detect these autism-associated language patterns. The researchers found that ChatGPT, zero-shot (without task-specific training), outperformed traditional machine learning models in classifying text as autistic vs. non-autistic language, and it highlighted telltale features like echolalia, pronoun reversal, and atypical speech as key indicators. Essentially, the LLM could read transcripts and reliably pick up subtle linguistic cues that a human diagnostician would note. This points to AI being used as a support tool for clinicians – for example, feeding an adult’s self-introduction or a child’s recorded speech into a model to get an analysis of whether it contains markers characteristic of ASD.
There’s also work on analyzing audio recordings of young children. Even without perfectly transcribing words, AI can assess vocal patterns – differences in prosody, tone, or the clarity of babbling. Some experimental tools use home video or microphone data and AI to flag if a 1-year-old’s babbling lacks the typical range of syllables or if their vocal turn-taking with a caregiver is unusual. In one notable project, smartphone videos of toddlers were analyzed by an AI which correctly identified a significant portion of autistic children long before a standard evaluation would. Another example is the NIH’s research on a prototype app that uses the phone’s camera and AI to track a toddler’s facial expressions and attention while they watch certain videos – early results showed it could successfully screen for autism by quantifying reduced social attention (like not looking at faces) and emotional reactivity.
By deploying these AI-driven analyses at scale (for instance, as part of routine pediatric care via an app), we could dramatically improve early detection, especially in communities with less access to specialists. An NLP-based system might analyze a simple questionnaire or even listen to a child’s attempt at words and give a risk score. This doesn’t replace a formal evaluation, but it can raise an early alarm so that families pursue a full assessment.
Enhancing Diagnostic Criteria with Big Data Insights
With enough data, AI might also help refine our definitions of autism. By analyzing thousands of cases, machine learning can uncover whether our current criteria optimally carve out the autistic population or if there are traits we’ve underappreciated. For example, one could feed an algorithm a wide array of symptom data from diagnosed individuals and see if it naturally clusters them – maybe it finds that there’s a cluster of children who all have severe sensory issues and motor stereotypies with only mild social problems, suggesting a potential subtype or a need to weight sensory symptoms more. In fact, the DSM-5’s inclusion of sensory sensitivities in ASD criteria was influenced by accumulating clinical evidence; in the future, data-driven approaches might further adjust criteria (e.g. how important is the presence of imagination/play deficits, or do we need to consider hyperactivity/impulsivity as a common associated feature?).
LLMs could also be used to parse longitudinal data – following how descriptions of a child change over time – to inform criteria about trajectories. For instance, maybe AI finds that those who clearly have ASD show a certain pattern by age 2 versus those who were late bloomers but not autistic. This could fine-tune screening checklists to reduce false alarms and false reassurance.
In essence, AI allows us to analyze autism not just case by case, but in aggregate at a scale never before possible. This helps find the signal in the noise of diverse presentations. It’s conceivable that future iterations of diagnostic manuals might be at least partly informed by such large-scale analyses, ensuring the criteria capture the most predictive and essential features of ASD identified through data.
Case Study: Folinic Acid and AI-Enhanced Insights
One especially intriguing example of AI’s utility is in making sense of research on folinic acid (leucovorin) treatment in autism. Folinic acid is a reduced form of folate (vitamin B9) and has gained attention due to findings that a subset of children with ASD respond to it with improved communication. However, these findings are nuanced – not every child benefits, and those who do often have specific biomarkers. Here’s how LLMs/NLP can help connect the dots:
Synthesis of Research Findings
The scientific literature on folinic acid in ASD spans case reports, small trials, and biochemical studies. A human trying to gather the gist would have to read through various papers: for instance, a 2013 study by Frye et al. showing many autistic children have folate receptor autoantibodies and respond to folinic acid; a 2016 randomized controlled trial showing folinic acid significantly improved verbal communication in children with ASD and language delays; follow-up meta-analyses in 2021 confirming the link between folate pathway abnormalities and autism; and perhaps anecdotal reports from clinicians. An LLM can ingest all these and produce a coherent summary:
For example, it might summarize: “Folinic acid at high doses (e.g. 2 mg/kg) has been found to improve language and social attention in a subset of children with ASD, particularly those with the folate receptor alpha autoantibody. In a double-blind trial, children receiving folinic acid gained ~5-7 points more in receptive and expressive language tests than placebo. Approximately one-third of treated children showed moderate or greater improvements in verbal communication and behavior. Children who were positive for folate receptor autoantibodies had the strongest response (large effect size). Side effects were minimal, similar to placebo.”
By citing the key numbers and outcomes from different studies, the LLM provides an evidence-based narrative that could be used by clinicians or included in guidelines. This saves enormous time and ensures no important study is overlooked due to human error.
Predicting Which Children May Respond
Crucially, not every child with ASD should be put on folinic acid; identifying responders is key. Research suggests responders often have biomarkers like FRAA (folate receptor alpha autoantibodies) or signs of cerebral folate deficiency (like low CSF folate). They might also have certain clinical features – for instance, some have drawn parallels to children with unexplained early regression or those with concurrent seizures and irritability (features hinting at a metabolic underpinning).
An AI model could be trained on data from folinic acid trials and case series: input features could include the child’s age, autism severity, presence of seizures, lab results (FRAA titers, perhaps MTHFR gene status, etc.), and whether they responded to folinic acid. The model could then predict for new cases the likelihood of response. For example, it might output something like, “Child with ASD who has high folate receptor antibody levels and a history of motor regression has an 80% probability of significant language improvement on folinic acid, whereas a child without those antibodies has a much lower probability.” Indeed, in Frye’s trial, FRAA status was predictive of response – FRAA-positive kids showed robust language gains on folinic acid vs placebo. An AI could generalize that: FRAA-positive → likely responder.
Furthermore, AI might find other predictors hidden in data. Perhaps children with certain genetic polymorphisms in folate metabolism (like MTHFR variants) or those with co-occurring mitochondrial dysfunction respond better. The 2021 systematic review indicated that 43% of ASD+CFD cases had mitochondrial dysfunction as a contributing factor, so maybe an AI would pick up that “if there are signs of mitochondrial issues (e.g. high lactate levels or fatigue), folinic acid might be especially beneficial.” These insights can form a precision-medicine approach: we could test children with ASD for a panel of markers (FRAA, perhaps mitochondrial markers, etc.), and if positive, prioritize folinic acid therapy.
LLMs can assist by reading through each patient’s record and flagging those markers. For instance, imagine an LLM that has been fine-tuned on medical texts: it could analyze a child’s lab reports and note “elevated folate receptor antibody titer” and then recommend, based on knowledge synthesized from literature, consider trial of folinic acid. It’s like a learned assistant that remembers the obscure connection between an antibody result and a treatment that a busy clinician might miss.
Identifying Metabolic and Genetic Subgroups
Using folinic acid effectively also means understanding which subgroup of ASD we’re dealing with. AI analysis of data has already outlined one subgroup: children with Folate Receptor Autoimmune Disorder, who have ASD features largely driven by low brain folate. These kids might even be considered as having both ASD and CFD – effectively a distinct phenotype. Another subgroup might be those with Rett-like features or regression who aren’t Rett (MECP2-negative) but actually have a folate transport issue – indeed, some infants with FOLR1 mutations initially present with developmental stagnation and autistic-like behaviors, and can be misdiagnosed as autism until the metabolic cause is found.
LLMs could help cluster patients by reading their histories. For example, they might differentiate: Group 1 – “ASD with early language regression, seizures, and FRAA-positive”; Group 2 – “ASD with no regression, FRAA-negative, likely idiopathic.” This first group clearly aligns with the folinic acid-responsive CFD subtype. The LLM’s output could be used to guide further testing – maybe the AI notes, “This child’s profile matches the pattern of cerebral folate deficiency (as seen in literature cases), recommend checking CSF folate or FRAA.” Essentially, it acts as a pattern-matcher across case reports.
In terms of genetic subgroups, AI could cross-reference a child’s genetic testing results with known folate-related genes. If a child has a rare variant of FOLR1 or DHFR, an AI that’s read biomedical databases could flag that as relevant to folate metabolism, suggesting folinic acid might be beneficial. Or if a child has FRα autoantibodies (which are not genetic but often co-occur with certain HLA types), the AI might know the statistics: e.g., “71% of children with ASD in studies have FRAA; if positive, strong consideration for folinic acid.”
In essence, AI and LLMs can serve as bridges between data and decision: they gather scattered clues (biomarker tests, genetic findings, symptom patterns) and map them onto an intervention (like folinic acid) backed by research. For caregivers and clinicians, this means a more tailored approach – instead of trying folinic acid in a trial-and-error way on every child (which isn’t practical or necessary), AI could help pinpoint those kids who are likely to shine with this supplement. This maximizes benefit, avoids unnecessary treatments for non-responders, and accelerates improvements for the right children.
Looking Ahead
The folinic acid story is just one case study. But it exemplifies how synthesizing knowledge with AI can propel forward a niche but important treatment avenue. LLMs can compress years of research into a concise rationale for when to use folinic acid, articulate it in accessible language for clinicians, and even help identify candidates from within a clinic’s patient population. As more treatments targeting specific autism subtypes emerge (be it nutritional, pharmacological, or behavioral), such AI-driven synthesis and prediction will be invaluable in delivering individualized medicine in autism – moving away from one-size-fits-all and toward the right treatment for the right subgroup at the right time.
AI-Driven Tools Transforming Autism Care (as of 2025)
The influence of AI isn’t just theoretical or in research – several concrete tools and platforms are already in use, aiding in autism diagnosis, tailoring therapy, and discovering biomarkers:
- Digital Diagnostic Aids: In 2021, the FDA authorized Cognoa’s Canvas Dx, an AI-powered app for diagnosing autism in young children. The system uses machine learning to analyze short home videos of the child’s behavior alongside parent and clinician questionnaires. It then assists pediatricians by indicating the likelihood of ASD, especially useful for kids under 5. Similarly, in 2022 the FDA cleared the EarliPoint Evaluation by EarliTec, which uses eye-tracking AI technology to detect autism in children as young as 16 months. During EarliPoint, a toddler watches videos of social scenes while a camera tracks their gaze; the AI software compares the child’s moment-by-moment looking patterns to a normative database. Deviations in how the child follows social cues (for example, not looking at characters’ faces or failing to track interactive motions) signal risk for ASD. These tools are game-changers in that they provide objective, quantifiable measurements – something traditionally lacking in autism diagnosis, which relied on subjective observation. By making earlier and more accurate diagnosis possible, such AI tools can get children into intervention sooner, which is critical for developmental outcomes.
- Therapy Personalization Platforms: A few emerging platforms use AI to match autistic individuals with the therapies or supports most likely to help them. For instance, there are AI-driven coaching systems that analyze a child’s progress in real time and adjust the therapy curriculum. One prototype system employs machine learning to monitor a child’s responses during ABA sessions (through video and therapist input) and can suggest when to move to the next learning goal or when the child isn’t engaging and a different approach is needed. While much of ABA programming is still manually guided, these AI augmentations aim to increase efficiency and effectiveness by ensuring the therapy is always at the right level of challenge. Another example is in social skills training for older children: AI chatbots and avatars are used to practice conversation, and NLP algorithms analyze the user’s social responses, giving personalized feedback. A platform called X2 (hypothetical name) might use a virtual reality environment where an autistic teenager rehearses, say, a job interview; the AI evaluates their eye contact (via VR headset sensors), voice tone (via speech analysis), and answers (via LLM semantic analysis), then coaches them on improvements. Such tools are still in development, but pilot studies show they help users gain confidence in social settings in a safe, controlled way.
- Biomarker Discovery Consortia: Large research initiatives, often with industry partners, are leveraging AI to sift through high-dimensional biomedical data for autism biomarkers. For example, the Autism Biomarkers Consortium for Clinical Trials (ABC-CT) has employed machine learning on EEG data to identify brain-wave patterns that distinguish ASD. AI can handle the gigabytes of EEG time-series data far better than human eyeballing – one algorithm found that certain EEG features during sleep correlated with language development in minimally verbal autistic children, suggesting a potential biomarker for who might benefit from language interventions. Another project uses deep learning on MRI scans (via the ABIDE dataset, a big repository of autism brain scans) to look for anatomical differences. While no singular “brain scan test” for autism exists yet, these models have found subtle differences in connectivity (how strongly certain brain regions sync up) that could one day serve as a diagnostic aid or subtype classifier.
- Genetic and Genomic Platforms: Given that over 100 genes are clearly linked to autism, identifying genetic subtypes is an ongoing need. AI tools help geneticists in two ways: variant interpretation and pattern recognition. Platforms using AI (like DeepVariant or MOON) help classify whether a genetic variant in a child is likely pathogenic (disease-causing) or benign by comparing it to databases and predicting its impact. This speeds up the process of pinpointing a genetic diagnosis for those ~20% of autistic individuals who have one (e.g. identifying a CHD8 mutation that would place a child in a specific subcategory of ASD with macrocephaly). Additionally, AI is used to find clusters of gene expression. For example, one machine learning study analyzed the gene expression profiles in blood of children with ASD versus controls and found a set of inflammatory genes that were consistently upregulated in a subgroup of ASD. This hints at an immunogenomic subtype which could potentially be targeted with anti-inflammatory strategies. By 2025, clinicians can use some of these insights: for instance, if genetic testing finds a variant of uncertain significance, an AI-backed report might say “this variant in a synapse gene is similar to other variants seen in autism”, helping doctors and families understand its relevance.
- Screening and Monitoring Apps: Outside the clinic, apps for parents employ AI to screen and monitor progress. There’s an app that listens to a toddler’s vocalizations at home and uses an AI model to quantify language development – it can flag if the child isn’t babbling or speaking as expected for their age (adjusted for multilingual homes, etc.), prompting an early hearing or autism evaluation. For children already diagnosed, some apps use the smartphone camera to record short videos of certain behaviors and then use computer vision to measure them. For example, tracking sleep patterns or night-time movement (as sleep problems are common in ASD) – AI can analyze motion sensor or video baby monitor data to alert if the child is waking frequently or engaging in self-injurious behavior at night. These kinds of tools give caregivers data-driven insights and peace of mind, and they can share the data with therapists to adjust support plans.
- Collaborative Research Platforms: On the research front, large language models themselves are being studied to generate hypotheses. A project might use an LLM to read all of PubMed’s autism papers and then ask it questions like, “What environmental factors have the strongest reported association with ASD?” The LLM could output: “Air pollution (particulate matter, traffic-related) has been frequently cited as a risk factor, and maternal infection during pregnancy has also emerged in multiple studies.” Researchers can then validate and design studies around these leads. Another imaginative use is simulating clinical trials: some groups have fed LLMs with data from prior trials and then “asked” the model to predict outcomes of a hypothetical new trial (for example, a new drug for social apathy in ASD), to help design better real trials.
It’s worth noting that as of 2025, many AI tools are supplementary – they augment human clinicians, not replace them. Ethical considerations like ensuring AI recommendations are transparent and avoiding bias are paramount (for instance, training data must include diverse populations so that tools work for all groups). But the trend is clear: AI is becoming an ally in the quest to understand autism’s complexities and improve the lives of those affected. From catching the diagnosis earlier, to tailoring therapies, to discovering hidden biological clues, AI-driven platforms are accelerating progress at an unprecedented rate. The hope is that in the coming years, these technologies will help deliver more personalized, effective care – ultimately enabling each autistic individual to reach their fullest potential, with support tuned to their unique profile.
Sources: Recent advancements are documented in FDA news releases, clinical studies demonstrating AI applications, and expert commentary on integrating AI into autism care. These underline how technology, when used thoughtfully, is opening new frontiers in our approach to autism.
Frequency questions and possible answers :
| Possible Questions | Possible Answers Summary |
|---|---|
| What’s the difference between CFD, Autism, Rett Syndrome, and general speech delay? | Provided a comprehensive comparative table highlighting key distinctions in etiology, symptoms, neurological features, genetic/metabolic markers, behavioral criteria, response to treatment, age of onset, and diagnostic tests. |
| Who first defined autism, and how have the criteria evolved historically? | Leo Kanner first defined autism (1943), and Hans Asperger contributed (1944). The DSM criteria evolved from strict (DSM-III, 1980) to broader (DSM-IV, 1994) and unified spectrum (DSM-5, 2013), emphasizing repetitive behaviors as core criteria due to neurological significance. |
| Why are repetitive behaviors essential in autism diagnosis (DSM-5)? | Repetitive behaviors are neurologically distinctive in autism, reflecting unique brain connectivity and sensory processing issues. They differentiate ASD clearly from social communication disorders. |
| How can Large Language Models (LLMs) help autism research? | LLMs analyze extensive research, identifying patterns in effective interventions (e.g., folinic acid), predicting treatment responses, and uncovering biomarkers and autism subtypes. They can also improve early detection and refine diagnostic criteria using large-scale data analysis and patient narratives. |
| How specifically can LLMs evaluate folinic acid as a potential autism treatment? | LLMs synthesize research findings on folinic acid efficacy, predict patient responsiveness based on biomarkers (e.g., FRAA), identify metabolic/genetic subgroups benefiting most, and help clinicians target personalized treatment effectively. |
| Which AI-driven tools/platforms are already used in autism diagnostics and therapy? | AI-powered tools like FDA-approved Cognoa Canvas Dx (behavioral video analysis), EarliPoint (eye-tracking), speech/language apps, and genetic biomarker platforms (e.g., DeepVariant) are now used. They help with early diagnosis, personalized therapy matching, biomarker discovery, and research collaborations. |
| How can AI and NLP technologies create better diagnostic systems for autism? | AI and NLP can analyze unstructured clinical notes, parent reports, and patient speech samples, identifying linguistic and behavioral patterns predictive of autism. This improves early, accurate, and objective diagnosis. |
| What diagnostic tests differentiate autism from conditions like CFD? | Autism is diagnosed behaviorally (ADOS, ADI-R). CFD diagnosis relies on biochemical tests (CSF 5-MTHF levels, serum FRAA antibodies), while Rett Syndrome involves genetic MECP2 testing. General speech delay involves excluding other diagnoses with hearing tests and language assessments. |
| What tests determine if a child might benefit from folinic acid? | Tests include checking serum folate receptor alpha autoantibodies (FRAA), lumbar puncture for CSF folate levels, and genetic screening for folate transport genes (e.g., FOLR1). Positive results strongly indicate potential benefit from folinic acid treatment. |
| How can AI help predict which children respond well to autism treatments like folinic acid? | AI analyzes patient data (biomarkers, genetics, clinical history) to predict which children are likely responders. It identifies key predictors (e.g., FRAA status, metabolic markers), guiding precision medicine decisions. |
Diagnostic and Treatment Guide for Autism-related Symptoms (Speech and General Delays) in about 3-Year-Old
| Concern | Reason / Explanation | Recommended Tests | Treatment / Management Options |
|---|---|---|---|
| 1. Microbial Issues (Gut bacteria imbalance) | Microbial overgrowth (yeast, bacteria, parasites) can cause neuroinflammation, behavioral issues (autistic-like), and speech delay. | – Comprehensive Stool Analysis (CSA) – Organic Acids Test (OAT, urine) | – Probiotics, prebiotics – Dietary interventions – Antifungal or antibiotic treatments (based on results) |
| 2. Cerebral Folate Deficiency (CFD) | Low folate in brain (even mild) strongly linked with autism-like symptoms and speech delays. Improvement after folinic acid strongly indicates CFD possibility. | – Serum Folate Receptor Alpha Autoantibodies (FRAA) (blood test) – Lumbar puncture for CSF 5-MTHF level (definitive test) – MTHFR Genetic Test (blood/saliva) – Brain MRI (to check brain structure, optional for supportive evidence) | – High-dose Folinic Acid supplementation |
| 3. Gluten and Milk Sensitivity (Dietary Issues) | Gluten (wheat) and dairy (casein) proteins may trigger gut inflammation and neurological symptoms, contributing to autistic behaviors and speech delays. | – IgE Allergy test (immediate reaction, blood) – IgG Food Sensitivity test (delayed reaction, blood) – Celiac Disease Panel (blood): Anti-tTG IgA, total IgA | – Gluten-free diet if positive – Dairy-free (casein-free) diet if positive |
| 4. Vaccine-related and Gut Inflammation | Some studies suggest immune response or inflammation post-vaccine may trigger gut dysbiosis, potentially affecting neurodevelopment (though controversial and not universally accepted). | – Immune panel (CBC, Ig levels, CRP, ESR) (blood) – Autoimmune markers (ANA, anti-brain antibodies, blood) – Heavy metals screening (urine or hair analysis) (controversial but used by some clinicians) – Stool analysis for inflammation markers (calprotectin, zonulin) | – Anti-inflammatory diet (GAPS or SCD diet) – Probiotic therapy – Detoxification protocols (gentle, supervised by physician) |
Additional Explanation: Why Folinic Acid Helps Your Child
Reason:
Folinic acid supports brain folate levels directly, bypassing potential folate transport issues (CFD). It aids mitochondrial function, reduces neuroinflammation, and enhances neurotransmitter production crucial for speech and cognitive development. Significant behavioral improvement strongly indicates underlying metabolic (folate transport or mitochondrial) issues responsive to folinic acid.