EEG in Young Children with Developmental Delays or Autism: What Can It Tell Us?
Children around age 2–4 who show developmental delays – for example, not responding to their name, language regressions, or other behaviors raising concern for autism – often undergo an electroencephalogram (EEG) as part of their evaluation. An EEG is a noninvasive test that records the brain’s electrical activity (“brain waves”) via sensors on the scalp . In clinical practice, EEGs are primarily used to detect epilepsy or abnormal brain activity, but they can provide clues if a child’s developmental issues might be related to neurological problems like seizures rather than (or in addition to) autism. This article will explain how EEGs are used in these young children, what the results can (and cannot) show, the types of EEG recordings available (30-minute routine EEG, sleep EEG, 24-hour EEG, etc.), and what different EEG abnormalities mean. We’ll also discuss whether episodes such as a child laughing for “no reason” could be seizures, and in the end, explore how modern AI and deep learning can help analyze EEG data to improve diagnosis for neurodivergent children.
Can an EEG Diagnose Autism or Developmental Disorders?
EEG cannot directly diagnose autism. Autism spectrum disorder (ASD) is a behaviorally defined condition – there is no specific brain-wave pattern on EEG that definitively identifies autism . Research has found certain group-level EEG differences in autistic individuals (such as differences in connectivity or brain rhythms), but these are not consistent enough for a clinical diagnosis . For example, some studies noted that children with ASD may show higher power in delta (slow wave) activity or altered connectivity in certain bands . However, a 2023 systematic review concluded that current EEG analyses “do not have the sensitivity or specificity needed to make a clinical diagnosis of ASD in children today.” In other words, many autistic children have normal EEGs, and some non-autistic children can have EEG abnormalities, so EEG alone isn’t a reliable test for autism.
That said, EEGs are still very useful in the evaluation of a young child with developmental delays or autism-like features. Doctors often order an EEG to look for other neurological issues (particularly epileptic activity) that might explain or contribute to a child’s language delay or regression. For example, a small percentage of children who initially present with autism-like regression actually have an epilepsy-related condition like Landau–Kleffner syndrome (also called acquired epileptic aphasia) or other epileptic encephalopathies. These conditions can cause a previously normal child to lose language skills or stop talking (much like autism regression) but are caused by abnormal brain electrical activity during sleep . In Landau–Kleffner syndrome (LKS), the EEG shows frequent spikes (especially in the temporal regions of the brain) and often nearly continuous epileptiform discharges during sleep, a pattern called ESES (electrical status epilepticus in sleep) . Identifying this pattern on EEG is crucial, because LKS is treated differently (with anti-seizure medications or steroids) and has a different prognosis than typical autism .
Moreover, autistic children have a higher chance of EEG abnormalities and seizures than the general population. Studies estimate that up to 20–30% of children with autism will develop epilepsy by adolescence, and even those without obvious seizures sometimes show “subclinical” epileptiform activity on EEG . One review noted that at least 15% of children with autism who have never had a seizure still showed spikes on EEG, compared to about 3% of neurotypical children . These spikes are often clinically silent (no outward seizure), but there is debate about whether they might contribute to developmental problems like momentary “staring” episodes or cognitive regression in some kids . For parents and doctors, finding an EEG abnormality might prompt closer monitoring for seizures or consideration of anti-seizure treatment if the EEG abnormalities are significant and correlated with developmental loss.
In summary, a normal EEG does not rule out autism, and an abnormal EEG does not prove autism – but the EEG can reveal if there is another brain issue (like epilepsy) co-occurring with autism or causing similar symptoms. Autism diagnosis remains based on developmental and behavioral evaluations, while EEG helps paint a fuller picture of the child’s neurological function.
What EEG Abnormalities Mean: A Guide to Common Findings
When an EEG is done (often a 30-minute awake recording initially), the results might come back as “normal” or “abnormal.” An abnormal EEG could show several types of findings. Here is a breakdown of some common EEG abnormalities, what they mean, and why they matter:
Generalized 3 Hz spike-and-wave discharges on EEG (marked by spike complexes repeating about three times per second). This classic pattern is seen in childhood absence epilepsy . Each spike is a brief epileptic discharge, followed by a wave. Such generalized epileptiform activity indicates a tendency for absence seizures.
- Epileptiform Discharges (Spikes, Sharp Waves, Spike-and-Wave Complexes): These are brief “spike” or “sharp” blips in the EEG waveforms that signify hypersynchronous neuronal firing. Seeing spikes or spike-and-wave patterns is a hallmark of a seizure tendency . If they appear in both hemispheres simultaneously (generalized), they may indicate a generalized epilepsy syndrome (for example, the 3 Hz spike-and-wave pattern in the image above is typical of absence seizures) . If spikes are localized to one area (focal spikes), they suggest a potential seizure focus in that region (for instance, spikes in the left temporal area might correlate with complex partial seizures arising from the left temporal lobe). A single, isolated spike might not be significant (even some healthy people have an occasional spike), but frequent or consistent spikes greatly increase suspicion of epilepsy . In children with developmental delays, the presence of epileptiform discharges – even without observed seizures – could indicate an “electrical” disruption of brain networks that might affect learning or language . For example, in Landau–Kleffner syndrome, frequent temporal lobe spikes during sleep interfere with language processing, leading to loss of speech .
- Electrical Status Epilepticus in Sleep (ESES): This is a severe form of epileptiform EEG abnormality where during slow-wave sleep the brain activity is almost continuously spiking. It is defined by a very high frequency of spike-wave discharges (often occupying >85% of each minute of NREM sleep) . ESES is seen in conditions like Landau–Kleffner and related epileptic encephalopathies. It means the brain is essentially in a constant epileptic state during sleep. Clinically, children with ESES often have regression in language, cognition, or behavior. If an EEG report mentions a “spike-wave index” (percentage of sleep occupied by spikes) that is extremely high, it may suggest this pattern. This abnormality would prompt aggressive treatment, as it can significantly impair development.
- Slowing of Brain Waves: Apart from spikes, EEGs might show slowing, which means the normal faster rhythms are replaced by unusually slow activity. Slowing can be generalized or focal. Generalized slowing (excess theta or delta waves across the whole brain) is a non-specific sign of diffuse cerebral dysfunction . It might occur if the child is drowsy or on sedating medicine during the EEG, but if the child was alert, generalized slowing could indicate factors like an underlying metabolic or structural issue, or simply reflect developmental delay or encephalopathy (brain “sluggishness”). Focal slowing, on the other hand, means one region (e.g. the left hemisphere or a specific lobe) shows slower waves than expected. This often points to a structural or localized brain issue in that area – for example, a focal cortical dysplasia, past injury, or other lesion could cause persistent slow waves over that region. In a 3-year-old with developmental delay, focal slowing on EEG might prompt imaging (like an MRI) to look for a structural cause in that part of the brain. In summary, slowing = possible dysfunction, with generalized slowing suggesting widespread effects (e.g. diffuse developmental issues or sedation) and focal slowing suggesting a problem in one area.
- Hypsarrhythmia: This is a very chaotic, high-amplitude mixture of slow and sharp waves, without a clear rhythm, and is the classic EEG pattern of infantile spasms (West syndrome). It’s mentioned here because if a very young child (typically under 2, but sometimes around 2–3) has developmental regression and an EEG report says “hypsarrhythmia,” it indicates an epileptic encephalopathy (infantile spasms) which can also present with developmental arrest or regression. Hypsarrhythmia is a medical emergency pattern – it looks like extremely disorganized brain activity – and requires urgent treatment. (The 30-minute routine EEG might or might not catch this; sometimes a sleep recording is needed.)
- Other Terms: EEG reports may mention other findings or normal variants. For example, “Mu rhythm” or “benign focal spikes” (also called benign rolandic spikes) can appear in children – these can be normal for age or benign childhood epilepsy markers. If an EEG is done awake in a drowsy 3-year-old, they might note “hypnagogic hypersynchrony” (a normal pattern in drowsy children) which is not a pathological abnormality. It’s always good to have the neurologist explain the report in plain language – which part is truly abnormal versus normal for the child’s age. Generally, the key abnormalities of concern in our context are the epileptiform discharges and significant slowing as described above.
Below is a summary table of some common EEG findings and their typical significance:
| EEG Finding | What It Means | Possible Implication |
| Spikes or Spike-and-Waves (epileptiform discharges) | Indicates irritable or seizure-prone area in the brain. Can be focal (localized) or generalized. The brain had a brief burst of abnormal synchronized firing. | High suspicion for epilepsy. If frequent, correlates with a risk of seizures. Specific patterns point to syndromes (e.g. 3 Hz generalized spike-wave = absence epilepsy). |
| Continuous Spikes in Sleep (ESES pattern) | Nearly constant spiking during slow sleep, often >85% of sleep EEG . | Suggests an epileptic encephalopathy like Landau–Kleffner or CSWS. Often associated with language or cognitive regression; needs prompt treatment. |
| Focal Slowing (e.g. delta waves over one region) | Local brain dysfunction in that area . Could be due to structural lesions or damage. Not an epileptic spike, but brain waves are sluggish in one spot. | Suggests looking for a structural problem (tumor, malformation, old injury) in that region. May correlate with developmental issues related to that brain area. |
| Generalized Slowing (slowed background rhythm) | Diffuse brain slow-down , lack of normal faster rhythms. Could be from sedation, drowsiness, or global brain dysfunction/immaturity. | If not due to sedation or sleep, may indicate global developmental or metabolic problems. Often seen in encephalopathies or significant developmental delay. |
| Normal EEG for age (no abnormalities) | Brain activity appears within normal limits for the child’s age. (Note: normal EEG doesn’t mean “no problem” – just no detectable electrical issue.) | No evidence of epilepsy or brain dysfunction on the EEG. The cause of developmental delay likely lies elsewhere (genetic, cognitive, etc., rather than overt epileptic activity). |
Table: Common EEG findings in young children and their significance. Keep in mind that EEG is just one part of the puzzle. For any individual child, these findings must be interpreted in context. For instance, a child with autism might have a few spikes on EEG that never lead to any seizures – or conversely, a child with a normal EEG could still have autism or other disorders. The EEG is a tool to pick up electrical issues, primarily.
Types of EEG Studies in Children (Routine vs. Sleep vs. Prolonged)
Not all EEGs are the same. Depending on the clinical question, neurologists might order different types of EEG recordings for a child:
- Routine Awake EEG (20–30 Minute Recording): This is the most common starting point. In a routine EEG, the technician applies ~21 electrodes to the child’s scalp (according to the standard 10–20 system). The recording itself lasts roughly a half hour to an hour (though setup adds extra time). During this time, the child is encouraged to be awake; standard “activation procedures” are often used to provoke any abnormalities – for example, the child might be asked to breathe fast (hyperventilate) for a few minutes (which can provoke absence seizures or slow waves), or be exposed to flashing lights (photic stimulation) to see if any abnormal response occurs . In children around age 3, hyperventilation may be done by encouraging the child to blow on a pinwheel or pretend to blow out candles. Photic stimulation involves a strobe light flashing at various frequencies with the child’s eyes closed. These procedures are safe and help increase the yield of the test . The routine EEG often also tries to capture the child getting drowsy or falling asleep if possible, because some abnormalities appear only in sleep . In fact, many pediatric EEG labs prefer to record both wake and sleep states in even a routine EEG . Parents might be instructed to partially sleep-deprive the child (e.g. put them to bed late or wake them extra early) so that the child will be more likely to nap during the EEG . The routine EEG is non-invasive and painless, though getting a toddler to sit still with wires on their head can be challenging! Sedation is avoided if possible (because it can suppress some forms of epileptiform activity), but if a child is extremely agitated, mild sedation might be used to obtain the recording .
- What it can diagnose: A routine EEG is good at picking up frequent epileptiform discharges or certain classic epilepsy patterns. For example, if a child has typical absence seizures dozens of times a day, a routine EEG might catch the 3 Hz spike-wave pattern. Or if a child has a tendency for focal seizures arising from one area, the interictal spikes might appear in a short recording. However, a routine EEG can miss infrequent abnormalities. If the child didn’t happen to have any discharges in that 30-minute window, the EEG will look normal even if they have epilepsy. Overall, the yield of a single routine EEG in children with suspected seizures is such that roughly 50% of people with epilepsy might show something on the first EEG. If it’s normal and suspicion remains, doctors sometimes repeat the EEG or do more prolonged monitoring.
- Sleep EEG or Sleep-Deprived EEG: This is basically an extended routine EEG with an emphasis on capturing natural sleep. For children who only had an awake EEG, the doctor might order a separate sleep EEG if they strongly suspect certain conditions (like Landau–Kleffner or benign focal epilepsy of childhood) that preferentially show abnormalities in sleep. In practice, many “routine” EEGs in pediatric centers already include sleep if possible . A true dedicated sleep EEG might involve bringing the child in at nap time or in a sleep-deprived state to almost guarantee they’ll conk out. The reason is that sleep can activate epileptiform activity – some EEG abnormalities only show up or dramatically increase during sleep . For example, the spikes associated with Landau–Kleffner syndrome can be rare in waking but become almost continuous in sleep. In one study, epileptiform abnormalities were found in 33% of children with language regression when prolonged sleep EEGs were done, versus only 16% on routine (mostly awake) EEGs . This shows how important a sleep recording can be when the awake EEG is normal but clinical suspicion is high.
- What it can diagnose: Sleep EEG is particularly useful for detecting nocturnal seizures or continuous sleep spiking (ESES). It can also catch patterns like benign centrotemporal spikes (rolandic spikes), which often occur in drowsiness or sleep. If a child is suspected of having subclinical seizures at night (e.g. waking up confused, or developmental regression worse in the morning), a sleep EEG is very helpful.
- Prolonged or 24-hour EEG (Ambulatory EEG): If a routine study is normal and questions remain, the next step might be a prolonged EEG recording. This could be done in the hospital or with an ambulatory EEG unit at home. An ambulatory EEG involves the child wearing a portable EEG recorder (with electrodes glued on the scalp and a little recorder box) for 1 to 3 days at home . Often a video camera is set up as well to correlate any events with the EEG. The goal is to capture events that happen infrequently – for example, if a child has a strange laughing episode once a day, a 24-48 hour recording stands a better chance of catching one than a 30-minute test . Ambulatory EEGs allow the child to be in their normal environment, sleeping in their own bed, which can be an advantage. In some cases, doctors schedule a short hospital admission for a 24-hour video EEG, particularly if they want continuous observation or need to ensure the study’s quality. During a prolonged study, the child can do normal activities (play, sleep, etc.), and if the parents notice any of the concerning behaviors (staring spells, laughing episodes, etc.), they press a button to mark the event.
- What it can diagnose: Prolonged EEGs are great for capturing rare events and quantifying seizure frequency. They increase the yield of finding any epileptiform discharges since there’s more recording time . For example, if seizures or spikes occur only during the night, a 24-hour study will catch the sleep hours. Ambulatory/home EEGs are often used when doctors suspect events like absence seizures that might happen a few times a day, or subtle events that parents aren’t sure about. They are also useful to see how often subclinical seizures or spikes are happening, which can help in treatment decisions . One limitation is that at home, if something happens, there isn’t a nurse right there – so some events might be missed on video if the child is off-camera. But many modern ambulatory EEGs are monitored remotely or checked periodically.
- Hospital Video-EEG Monitoring (Long-Term Monitoring): For very complex cases or if high diagnostic certainty is needed, a child might be admitted to an Epilepsy Monitoring Unit (EMU) for multiple days of continuous video-EEG. This is the most intensive monitoring. The child is in a hospital bed with EEG on at all times and a camera recording them. Technologists and nurses can observe in real time. Sometimes doctors will intentionally sleep-deprive the child further or even taper off medications (in a controlled setting) to provoke events . This is usually done for children who have hard-to-capture events or when considering epilepsy surgery (to pinpoint seizure focus) – it might be beyond the needs of a child who just has developmental delay without clear seizures. The advantage in the hospital is safety (IV medications on hand if a big seizure occurs) and ensuring any event that happens is recorded clearly on video and EEG .
- What it can diagnose: It can conclusively tell if an event is a seizure or not, capture even rare seizures by extending days until one occurs, and localize seizures precisely. For our discussion (non-verbal/autistic toddlers), inpatient EEG is rarely needed unless there are uncontrolled seizures or diagnostic confusion after outpatient studies.
In practice, the workup might go stepwise: Start with a routine EEG (with sleep if possible). If that’s normal but concern for epilepsy remains, do a sleep-deprived EEG or ambulatory EEG. In cases of regression where Landau–Kleffner is a concern, often a sleep EEG or even an overnight EEG is done early, because the sleep portion is critical to see the characteristic pattern . Always discuss with the pediatric neurologist what type of EEG they are ordering and why – understanding the test can help parents prepare the child (like keeping them up late before a sleep-deprived EEG!).
Unexplained Laughing Spells in a 3-Year-Old: Could It Be Seizures?
A concerning scenario some parents report is their toddler having episodes of laughing or giggling for no apparent reason, often in a stereotyped way. While children certainly can laugh when feeling happy or even giggle randomly, frequent “laughing attacks” that seem inappropriate to the context can indeed be a type of seizure known as a gelastic seizure. “Gelastic” comes from the Greek word for laughter.
Gelastic seizures are seizures that manifest as bouts of laughter or laughing-like vocalizations, usually without any clear trigger and often with an unusual, forced quality . During such a seizure, the child may appear momentarily strange – they might suddenly laugh or smile, perhaps with a far-off look in their eyes, and it’s not because of anything funny. The laughter typically sounds not like a joyful belly laugh but more mechanical or empty, and the child cannot control it . These episodes are usually brief (often 10–20 seconds) . In infants and toddlers, parents might notice the child’s laughter is different – for instance, a baby waking up with a strange chuckle periodically.
One classic cause of gelastic seizures is a benign tumor in the brain called a hypothalamic hamartoma, which is present from birth in some children. This lesion in the hypothalamus often triggers laughter seizures in infancy or early childhood . A child with hypothalamic hamartoma might have dozens of these giggling episodes per day. In fact, gelastic seizures “can occur many times a day – in some cases, as many as 100 a day” . Over time, children with this condition may develop other seizure types or developmental issues if untreated .
How do you tell a gelastic seizure from just goofy toddler behavior? Key things to look at: the frequency and stereotyped nature of the episodes, and the child’s awareness. If for example a 3-year-old occasionally breaks into laughter because they thought of something funny or are seeking attention, it’s usually situational and the child can be engaged during it. In a gelastic seizure, the laughter is often unprovoked (happening out of the blue) and may have a distinctly repetitive pattern (same duration, same quality each time). The child may not respond normally during it – for example, you call their name and they don’t seem to fully register because they are in a seizure. Afterwards, they carry on as if nothing happened, or sometimes seem briefly confused. Gelastic seizures commonly happen as the child is falling asleep or waking (but can happen anytime) . Parents might notice, “Every night just as he’s dozing off, he suddenly lets out this peculiar chuckle and his eyes stare – then it’s over.”
If you suspect these laughing episodes are seizures, it’s important to bring it up with the pediatrician or neurologist. The doctor will likely order an EEG and an MRI of the brain. EEG and gelastic seizures: Interestingly, gelastic seizures can be tricky to catch on EEG. Because the hypothalamus (where the hamartoma is) is deep in the brain, the scalp EEG might not show a big obvious spike during a short laughing seizure . Routine EEGs can even be normal in children with gelastic seizures . Often, the diagnosis is made by the clinical story plus an MRI finding of the hamartoma. However, if the child has other seizures or the gelastic seizures generalize (spread to the whole brain), the EEG can show corresponding changes.
The bottom line: “Laughing for no reason” in a repeated, stereotyped way is a red flag for gelastic epilepsy. These seizures are rare, but awareness is crucial because they often go unrecognized for a long time . Many parents don’t initially think a laughing spell could be a seizure, and even doctors might misattribute it to behavioral issues. If a child has frequent daily episodes of unexplained laughter (or crying, in the case of dacrystic seizures which are crying seizures), a thorough neurological evaluation is warranted. Treatment of gelastic seizures (especially due to hypothalamic hamartoma) may involve medications, and in some cases, surgery or laser ablation of the hamartoma to stop the seizures.
How AI and Deep Learning Are Improving EEG Diagnosis
Interpreting EEGs and linking patterns to specific diagnoses is a complex task – one that traditionally relies on the expertise of neurologists and electrophysiologists. However, the rise of artificial intelligence (AI) and deep learning is starting to transform this field. For children with developmental disorders, AI holds promise in a few major ways:
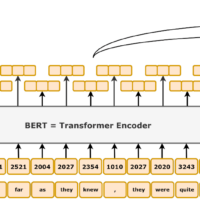
- Early Autism Detection from EEG: While EEG isn’t a clinical diagnostic tool for autism yet, researchers are using machine learning to find subtle biomarkers. Remarkably, a study by researchers at Boston Children’s Hospital and others found that using machine learning on infant EEG data could predict later autism diagnosis with high accuracy . They recorded EEGs from babies as young as 3 months old who had a high family risk of ASD, and by analyzing nonlinear EEG features and feeding them into a predictive model, they achieved over 95% sensitivity and specificity in distinguishing which babies would later be diagnosed with autism . This kind of result suggests there are hidden patterns in brain activity that the human eye can’t easily see but algorithms can. In the future, EEG combined with AI might become an early screening tool – imagine a scenario where a 6-month-old’s EEG, analyzed by a computer model, flags a high likelihood of ASD, prompting earlier behavioral interventions even before symptoms are overt. We’re not there in routine practice yet, but research is rapidly advancing . In fact, all studies do find differences in EEG between ASD and non-ASD – it’s just that individual variation is high . With larger datasets and refined algorithms, consistency may improve. AI could also help subtype autism: for instance, distinguishing an EEG pattern more common in autistic children with language regression versus those without – leading to more personalized interventions.
- Seizure Detection and EEG Monitoring: One of the most practical applications of AI in EEG is automatic seizure detection. Algorithms (including deep neural networks) can be trained on thousands of hours of EEG to recognize the signature of a seizure. In pediatric epilepsy monitoring, AI systems are already being used to alert doctors that “a seizure is happening” by analyzing incoming EEG in real time. A 2024 systematic review showed that machine learning methods for detecting pediatric seizures from EEG have high accuracy – with deep learning models achieving around 89–91% accuracy and similarly high sensitivity and specificity in identifying seizures . This is comparable to expert humans and greatly speeds up EEG analysis, especially for long recordings. For parents, this means in the future ambulatory EEG devices might come with AI that alerts you on a smartphone if your non-verbal child is having an EEG change suggestive of a seizure (useful for silent seizures at night, etc.). In hospitals, it means busy ICU staff can be notified of a seizure without waiting for an EEG specialist.
- EEG Pattern Recognition for Diagnosis: Beyond seizures, AI can sift through EEG data for other patterns – maybe detect those subtle focal slow waves that a human might miss, or quantify the percentage of sleep with spikes (spike-wave index) more objectively than a human. This can help diagnose conditions like ESES more quantitatively and earlier. AI might also help differentiate, say, an EEG pattern of metabolic encephalopathy from an EEG pattern of an epileptic encephalopathy, by recognizing complex features across frequencies that are hard for a person to integrate mentally. For children who are non-verbal or cannot communicate symptoms, such automated insights are especially valuable.
- Building EEG Databases for Prediction: The question posed the idea of each clinic building a dataset of EEGs with the child’s history/outcome to train AI. This is indeed how many advances happen – by pooling data. If many hospitals contribute anonymized EEG recordings of children along with their diagnoses (autism, LKS, ADHD, etc.), researchers can develop algorithms to find correlations. The larger and more diverse the dataset, the better the AI generally performs. This could lead to decision-support tools: for instance, an EEG of a 3-year-old non-verbal child could be run through an algorithm that says, “this EEG has patterns most similar to those from children with idiopathic autism, with a 5% chance of undiagnosed seizure activity”, or vice versa “this EEG is showing features often seen in Landau–Kleffner syndrome – consider further epilepsy evaluation.” Such tools would not replace doctors, but would augment their ability to diagnose, ensuring nothing is overlooked. As one review put it, EEG-based algorithms are “a crucial addition to other technologies… supporting early diagnosis” . They may especially indicate when a child needs deeper evaluation or faster referral, which is critical in neurodevelopmental disorders where early intervention matters .
- Personalized Therapy and Monitoring: AI can also help in treatment by analyzing EEG trends over time – for example, automatically tracking if the frequency of subclinical spikes is decreasing with a certain medication. In autism research, if EEG could delineate subtypes, it might influence therapy choices (this is speculative but possible in the long run).
It’s an exciting frontier. Importantly, for AI to truly help children, it requires collaboration: neurologists, data scientists, and large volumes of data. Privacy and ethics are paramount when dealing with children’s data, so any EEG dataset must be handled carefully (fully de-identified). Many parents are very willing to contribute data if it might help figure out their child’s condition or help others. In the near future, we can expect to see more AI-integrated EEG machines and diagnostic reports that include algorithmic analyses alongside the doctor’s interpretation.
Conclusion
For parents and clinicians navigating the challenges of a young child with developmental delays, language regression, or autism spectrum behaviors, EEG is a valuable piece of the puzzle – but not the whole puzzle. A normal EEG can be reassuring that no obvious epilepsy is present, while an abnormal EEG can reveal hidden factors like subclinical seizures or atypical brain activity that might be affecting the child’s development. We discussed how specific EEG patterns (spikes, slow waves, etc.) can point to conditions that sometimes mimic or accompany autism (like Landau–Kleffner syndrome or other epileptic encephalopathies) and why capturing sleep EEG is often key in such cases. We also addressed the curious case of gelastic (laughing) seizures – a reminder that not all unusual behaviors in neurodivergent children are “just behavioral,” and some warrant neurological evaluation.
Crucially, EEG results must be interpreted in context. An abnormal EEG doesn’t doom a child – it provides a target for treatment (for example, using anti-seizure medication to try to improve a child’s learning if they have a lot of epileptiform activity). And a normal EEG doesn’t mean the child’s challenges aren’t “real” – it simply means the cause lies beyond the kind of brain electrical disturbances EEG can detect. As always, the partnership between parents and healthcare providers is important: discussing why an EEG is ordered, what the results mean, and the next steps.
Finally, the advent of AI and deep learning offers hope for making sense of the mountains of EEG data in a way no human could on their own. From possibly detecting autism risk in infancy to greatly improving real-time seizure monitoring , these technologies are poised to assist doctors and empower patients. Imagine each EEG not as just squiggly lines read by one specialist, but as a source of data that, combined with thousands of other EEGs, can yield actionable insights – this is the vision of the future. By building large, diverse datasets and applying smart algorithms, we can move toward earlier and more accurate diagnoses for conditions like autism or epilepsy in children who cannot speak for themselves. In the end, the goal is better outcomes: a child who gets the right diagnosis and support as early as possible. EEG, both through traditional analysis and AI enhancement, is an important tool to achieve that goal.
Sources: The information above is drawn from current pediatric neurology research and clinical guidelines, including studies on EEG features in autism and regression , best practices for pediatric EEG recording , as well as expert resources from epilepsy organizations . Advances in AI are referenced from recent scientific reports on machine learning applied to EEG in autism and epilepsy . These resources are cited throughout the text for further reading.